Case study - Pediatric urinary tract infection: Nursing
Case study - Pediatric urinary tract infection: Nursing
NUR 231 Peds
NUR 231 Peds
Notes
| CASE STUDY - PEDIATRIC URINARY TRACT INFECTION (UTI) | ||
| KEY POINTS | NOTES | |
| INTRODUCTION |
| |
| RECOGNIZING AND ANALYZING CUES |
| |
| PRIORITIZING HYPOTHESES, GENERATING SOLUTIONS, AND TAKING ACTIONS |
| |
| EVALUATING OUTCOMES |
| |
Transcript
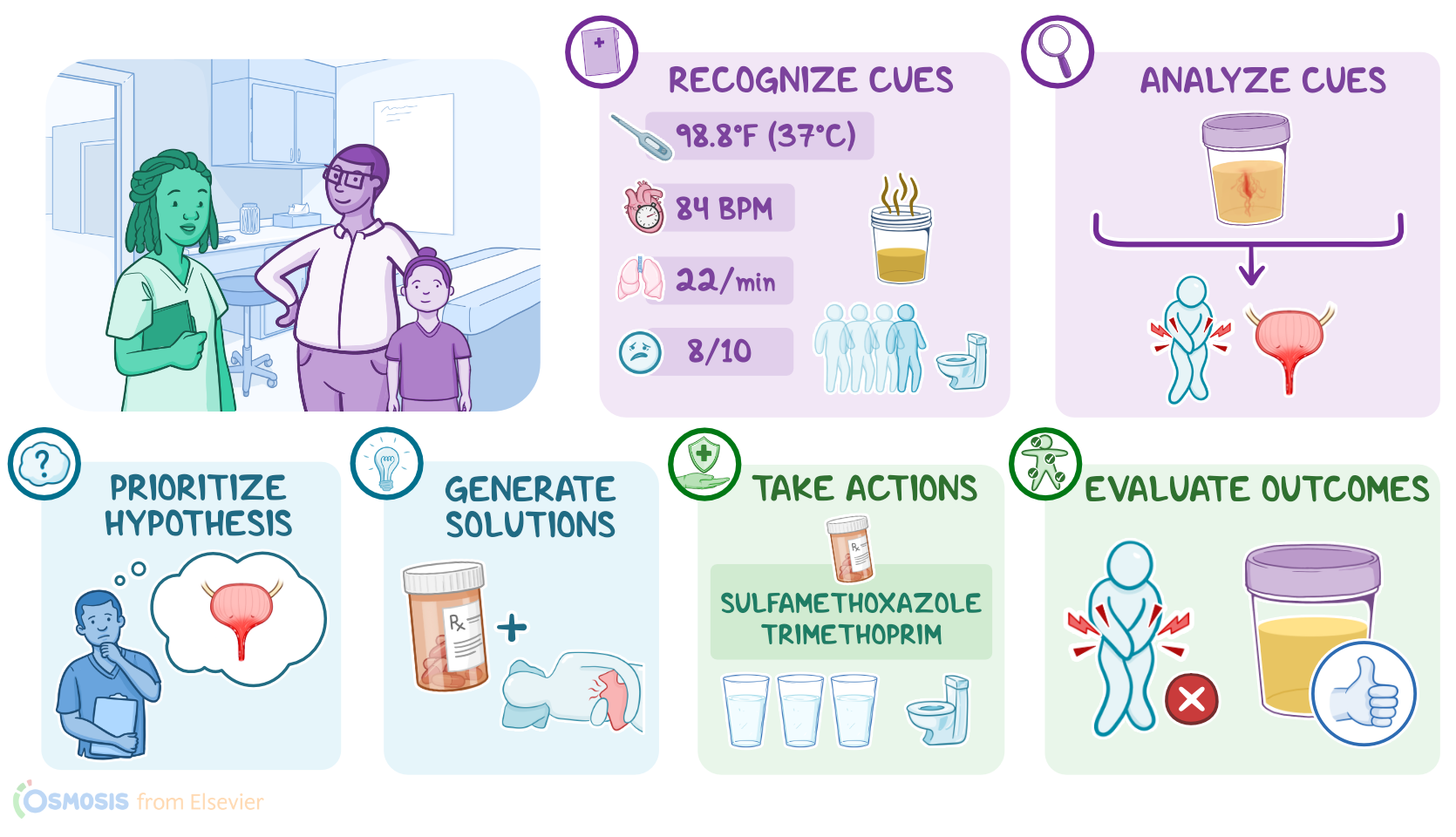
Nurse Michelle works at a pediatrician’s office and is caring for Emma, a fully toilet trained, 5-year-old female brought in by her father, Jim, for urinary frequency and crying when urinating. After settling Emma and her father in a room, Nurse Michelle goes through the steps of the Clinical Judgment Measurement Model to make clinical decisions about Emma’s care by recognizing and analyzing cues, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes.
First, Nurse Michelle recognizes important cues, including vital signs, which are temporal temperature 98.8 F or 37 C, heart rate 84 beats per minute, and respirations 22 breaths per minute; as well as Jim’s description of Emma’s dark, amber-colored, and foul-smelling urine. Jim also reports Emma has been urinating more often than usual. Emma rates her pain during urination an 8 out of 10 on the Wong-Baker FACES pain scale. Then, Nurse Michelle obtains a clean catch urine sample from Emma for dipstick urinalysis and assesses for suprapubic and flank pain, which revealed mild discomfort with palpation over the suprapubic area.
Next, Nurse Michelle analyzes these cues. She reviews the results of the urinalysis which shows positive for leukocytes, nitrites, and blood. Nurse Michelle recognizes that normal urinary elimination involves a controlled, painless release of urine that's typically light to dark yellow in color, transparent, with a slight odor, with no evidence of bacteria or blood. Nurse Michelle realizes Emma is experiencing altered urinary elimination. She shares her assessments with the health care provider who diagnoses a urinary tract infection.
Using information she's gathered along with Emma’s medical history, Nurse Michelle chooses a priority hypothesis of urinary tract infection.
Then, she generates solutions to address Emma’s infection that will include pharmacologic and nonpharmacologic interventions, and she establishes the expected outcome that after intervening: My patient will urinate without pain or frequency within one week.
Nurse Michelle then takes action to implement these solutions. She gathers information on the prescribed antibiotic as well as educational materials about preventing urinary tract infections, and re-enters Emma’s room.
Nurse Michelle: Emma, your health care provider is giving you some medicine that'll make it stop hurting to use the bathroom, okay? I’m also going to talk with you and your dad about ideas to help keep this from happening again. Does that sound good?
Emma: Yes.
Nurse Michelle: Okay, great. So, the medication Emma’s prescribed is called sulfamethoxazole trimethoprim. It'll clear up the urinary tract infection that’s causing her pain and frequency symptoms, but it can cause nausea, so you should give it with food. Give her 5 milliliters twice each day for 10 days.
You’ll use this little measuring cup to make sure you measure out the exact amount. Emma should start to feel better in a few days, but it’s important to finish all 10 days of the medicine so the infection doesn’t return.
Sources
- "Fundamentals of nursing (11th ed.)" Elsevier (2023)
- "Fundamentals of nursing: Active learning for collaborative practice (3rd ed.)" Elsevier (2022)