Complete blood count (CBC) - Hemoglobin and hematocrit: Nursing
Complete blood count (CBC) - Hemoglobin and hematocrit: Nursing
Watch later
Watch later
Notes
| HEMOGLOBIN AND HEMATOCRIT | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
A client comes to the outpatient clinic and reports feeling fatigued, weak, and is experiencing frequent palpitations. On assessment, the client’s skin and mucous membranes look pale and their extremities feel cold. Based on these findings, a complete blood count, or CBC, is ordered to check their hemoglobin and hematocrit.
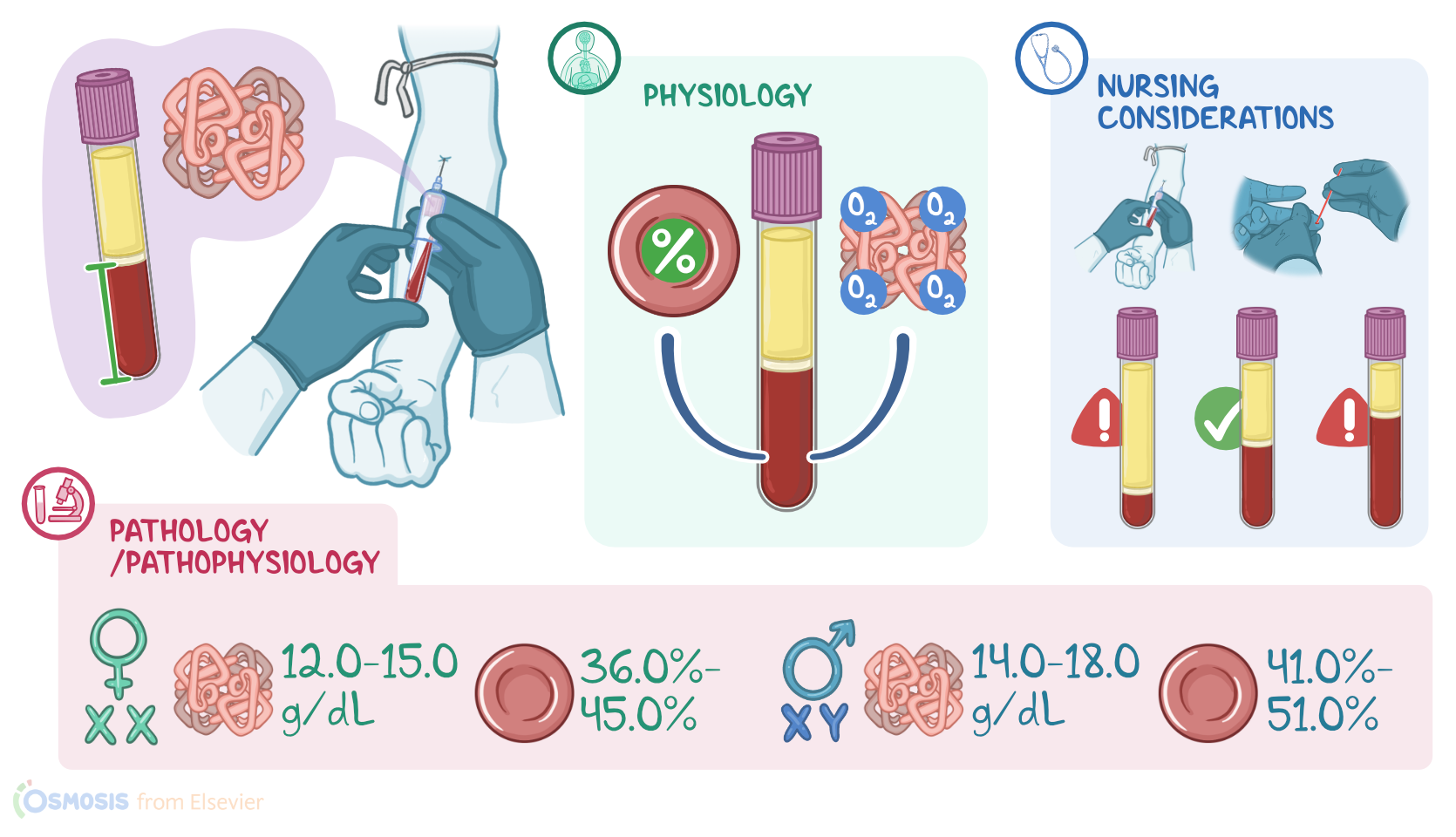
Now, hemoglobin, abbreviated as Hgb or Hb, and hematocrit abbreviated as Hct or sometimes Crit, are usually measured as part of a CBC, and they provide an indirect way to measure red blood cells or RBCs. Hemoglobin is an iron-containing protein found in RBCs, which allows them to carry oxygen from the lungs to peripheral tissues. The hematocrit represents the percentage of packed RBCs, also referred to as the Packed Cell Volume or PVC, in whole blood, that’s obtained after centrifuging part of the sample to allow for complete sedimentation of the RBCs.
The normal values of hemoglobin and hematocrit differ between the sexes. This is because in females, RBC production is stimulated by erythropoietin only, while in males, androgens provide additional stimulation for RBC production. So, in adult males, hemoglobin normally ranges from 14.0 to 18.0 g/dL, while in adult females it normally ranges from 12.0 to 15.0 g/dL. Hematocrit in males ranges from 41.0% to 51.0%, while in females it ranges from 36.0% to 45.0%.
Typically, the hematocrit will be about three times the value of hemoglobin. As an example, if a client’s hemoglobin is 14.0 g/dL, their expected hematocrit would be about 42%.
Alright, there are certain conditions that can alter a client’s hemoglobin and hematocrit.
When the number of RBCs increases, like in polycythemia vera, a condition where the bone marrow produces too many RBCs, hemoglobin also increases. These additional cells also increase the percentage of RBCs, which means that the hematocrit will go up as well.
Alternatively if the amount of fluid in the blood decreases, like with dehydration, the concentration of RBCs increases, and the hemoglobin and hematocrit will also increase.
In contrast, low levels can be caused by chronic blood loss due to conditions like peptic ulcer disease or heavy menstrual bleeding; decreased RBC production caused by certain hemoglobinopathies; or increased RBC destruction, which can happen with certain autoimmune disorders.
Another way hemoglobin and hematocrit can decrease is from fluid overload, where excess intravascular fluid dilutes the blood, causing a relative decrease in RBCs, and is referred to as dilutional anemia.
This occurs during pregnancy, where blood plasma increases more in relation to RBCs, in which case it’s referred to as physiological anemia of pregnancy.
Now, a client’s hemoglobin and hematocrit will be measured when there are signs or symptoms of low or high RBCs. If RBCs are low, signs and symptoms can include fatigue, weakness, pallor, cold extremities, tachycardia, palpitations, and chest pain.
On the other hand, symptoms of increased RBCs can include fatigue, dizziness, frequent nose bleeds, and itching after a warm shower.
Additionally, there are other scenarios where hemoglobin and hematocrit are measured. It can be used to assess a client recovering from surgery, as well as after an acute hemorrhage or episode of hemolysis. Finally, hemoglobin and hematocrit are measured to screen clients who are at risk for anemia.
Alright, let’s look at the nursing implications for a client with an altered hemoglobin or hematocrit. Your priority goals of care are to address the underlying cause, and to monitor your client’s hemoglobin and hematocrit levels.
First, collect a sample by venipuncture using a lavender-topped tube. This tube contains the anticoagulant EDTA to help prevent clotting of the sample.