For most mononeuropathies that have an acute presentation, the underlying cause may be difficult to define since they often resolve rapidly and provide no opportunity for a complete examination. Nonetheless, mononeuropathies are usually the result of local nerve damage caused by compression-related events that are classified as either fixed or transient.
Fixed mononeuropathies are mainly induced by nerve compression against a hard surface, such as a tumor, cast, or even a prolonged cramped posture (e.g., during hospitalization or surgery). As a result, there may be a change in sensation, and sometimes, in movement, of the affected area. Fixed mononeuropathies usually affect superficial nerves like the radial nerve, which extends along the forearm, or the peroneal nerve, which extends into the lower leg. Fixed mononeuropathies are more often noticed in very thin people, as the direct compression of nerves against bones can lead to the condition.
The continuous pressure that causes fixed mononeuropathies can progressively thin the myelin sheath, the protective cover of the nerve, through a process called segmental demyelination. If the pressure is persistent, it may cut through the myelin sheath and injure the nerve axon. This is referred to as Wallerian degeneration, and it can also occur due to local injury, like a deep cut through a nerve.
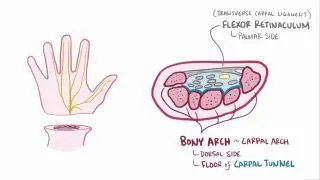
Additionally, the entrapment of nerves in narrow anatomical spaces can cause fixed mononeuropathies. For example, carpal tunnel syndrome describes when the median nerve is trapped, and cubital tunnel syndrome is when the ulnar nerve is trapped. Multiple risk factors can lead to the entrapment of a nerve in a restricted anatomical structure, including pregnancy and hypothyroidism (i.e., low levels of thyroid hormones), as well as rheumatoid arthritis, which causes swelling and stiffness of the affected joints.
Contrary to fixed mononeuropathies, transient mononeuropathies are triggered by repetitive actions that cause trauma, like aggressive muscular activity or sudden overextension of a muscle.
In some cases, mononeuropathies can be linked to non-compression related causes. Sometimes, exposure to cold or radiation may cause damage to a single nerve. Infections localized to an individual nerve, like
herpes zoster, can also lead to
mononeuropathy. Rarely, early
HIV infection can cause mononeuropathy expressed as
facial palsy, which usually improves spontaneously.