Diphtheria: Nursing
Definitions & Key takeaways
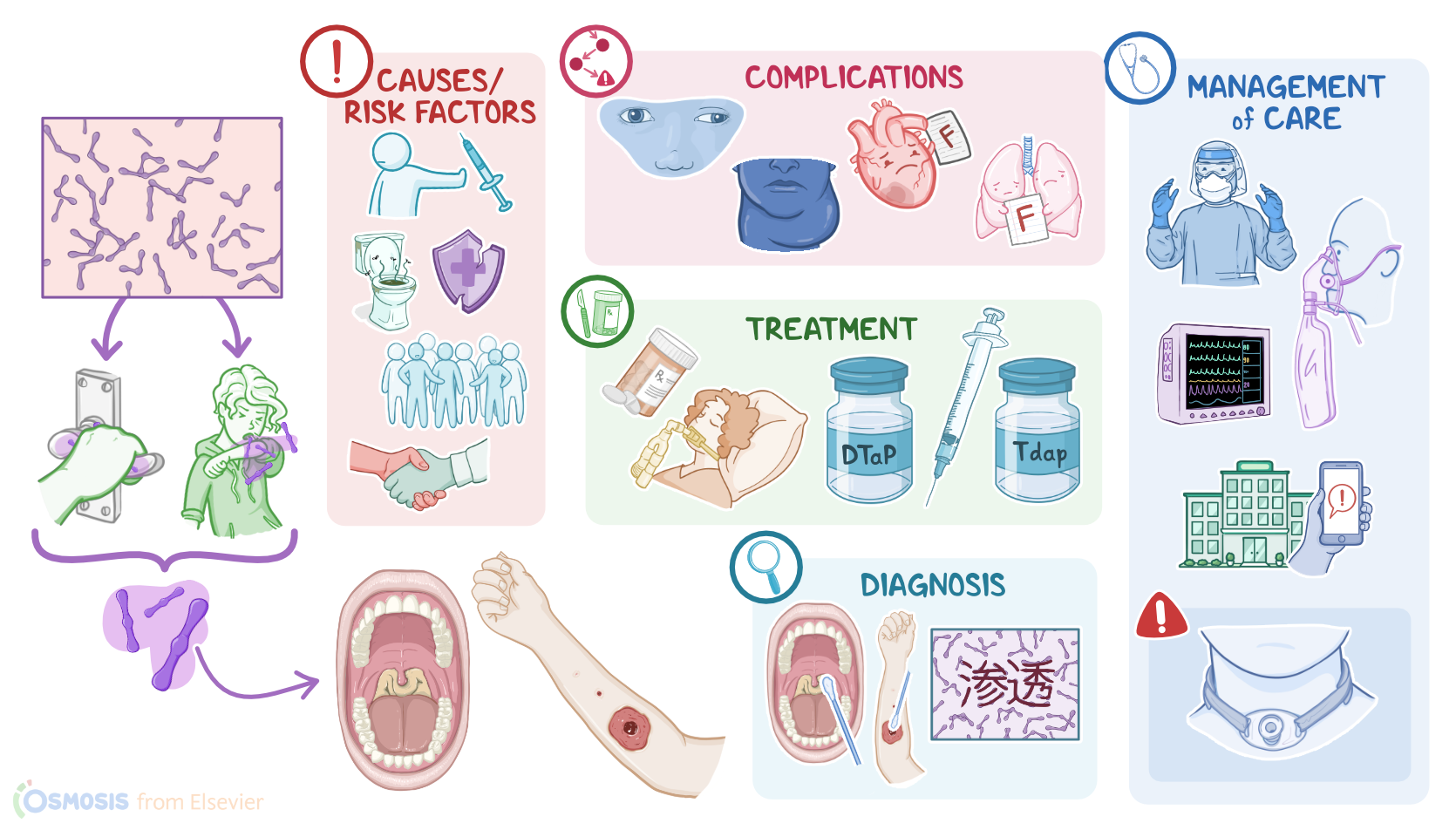
Diphtheria is a toxin-mediated infection caused by the bacterium Corynebacterium diphtheria. It primarily affects the nose and throat but can also spread to other body parts, causing severe respiratory illness or heart problems. Diphtheria is most commonly spread through respiratory droplets, such as when infected people cough or sneeze. The infection can also be spread through contact with contaminated surfaces, such as doorknobs or toys.
Diphtheria can be deadly if not treated promptly. Symptoms of diphtheria include sore throat, fever, chills, and grayish pseudomembrane on the posterior pharyngeal wall, which can make it difficult to breathe. Diphtheria is preventable through vaccination.
Introduction0:00–0:01
Introduction0:01–0:13
Diphtheria is a toxin-mediated bacterial infection that typically affects the upper respiratory tract, and less commonly, the skin.Now, let’s quickly review a bit of the anatomy and physiology of the upper respiratory tract, and skin.
Physiology0:13–1:54
Starting with the upper respiratory tract, this is made up of the nose, nasal cavity, oral cavity, pharynx, epiglottis, larynx, and the upper part of the trachea.
So, when we breathe in, air enters the respiratory tract through the nose or mouth, respectively into the nasal cavity and oral cavity, and then into the pharynx.
Zooming in, the epithelium lining respiratory tract consists of goblet cells that release mucus, which is sticky and contains enzymes to help trap and destroy harmful foreign particles and pathogens; as well as columnar epithelial cells, that have hair-like projections called cilia, which work to sweep the harmful particles up and out of the airways.
Moving on to the physiology of the skin, this is divided into three main layers: the hypodermis, which is made of fat and connective tissue, the dermis, which contains hair follicles, sweat glands, nerve endings, and blood vessels, and finally, the epidermis.
The epidermis itself has multiple layers of squamous or flat epithelial cells.Alright, now, diphtheria is caused by the gram-positive bacillus bacteria called Corynebacterium diphtheriae.
Causes & risk factors1:54–2:22
Important risk factors for developing diphtheria include immunodeficiency; being unvaccinated or undervaccinated; coming in contact with an infected client; and finally, living in crowded or unsanitary conditions or traveling to an endemic area.Moving on to pathology, Corynebacterium diphtheriae is an airborne bacteria, meaning it most often spreads via small bacteria-containing respiratory droplets that get flung in the air when an infected client talks, coughs, or sneezes.
Pathology2:22–4:36
If another client breathes in these droplets, or they get in contact with infected surfaces, and then touch their eyes or mouth, they can become infected with what is known as respiratory diphtheria.
Less frequently, the bacteria can also enter the body through open lesions on the skin, causing cutaneous diphtheria.Now, when infected by a beta bacteriophage, C.
diphtheriae becomes toxigenic, meaning that it is able to produce diphtheria toxin, or DT for short. So, once the bacteria enters the body, a subunit of the toxin binds to the epithelial cells lining the upper respiratory tract, particularly the pharynx, or tonsils, and less commonly, the skin.
In any case, the toxin proceeds to block protein synthesis, effectively causing the cell to die. This causes local inflammation that leads to tissue swelling, and necrosis.
Ultimately the necrotic tissue builds up into a gray, leathery pseudomembrane. The most common complication of diphtheria is obstruction of the airway that can lead to respiratory failure.
Additionally, the bacteria may gradually invade deeper into the wall of the respiratory tract or the skin, until they reach the bloodstream, from where they can move to distant organs such as the heart, causing myocarditis, or the kidneys, causing acute tubular necrosis, or destruction to the renal tubules.
C. diphtheriae can also travel to the nerves, causing nerve demyelination, meaning they destroy the myelin sheath covering the nerve axons, leading to polyneuropathy.
Diphtheria polyneuropathy usually affects the oculomotor nerve, causing oculomotor nerve palsy.Now, the clinical manifestations of diphtheria often begin to present 2 to 5 days after infection and include a low-grade fever accompanied by a general malaise and weakness.
Clinical manifestations4:36–5:37
In respiratory diphtheria, clients present with a sore throat, a swollen neck that’s commonly called bull neck, and a thick, gray, adherent coating called a pharyngeal pseudomembrane, which ultimately can cause difficulty breathing and stridor.
A barking cough and hoarseness are also often present.In cutaneous diphtheria, there are typically chronic skin ulcers, covered with a dirty gray membrane.
With myocarditis, there might be signs of cardiac dysfunction such as arrhythmias, or even heart failure. With acute tubular necrosis, there can be oliguria, or decreased urine production.
Finally, clients with oculomotor palsy may experience double vision.Diagnosis of diphtheria starts with the client’s history and physical assessment, followed by cultures of swabs from the pharynx or the suspected skin lesion to isolate C.
Diagnosis5:37–6:09
diphtheriae. When placed on a gram-stain, gram-positive rods appear in a “Chinese-character” looking distribution.
When the culture gets positive, next is to tell if the C. diphtheriae strain in question is toxigenic.
This can be done by a polymerase chain reaction or PCR or a rapid enzyme immunoassay.Treatment for diphtheria includes antibiotic therapy with erythromycin or penicillin.
Treatment6:09–7:21
Careful airway management, with early intubation and oxygen supplementation, is also necessary due to the risk of airway obstruction.
Additionally, all close contacts who are not up to date on vaccinations, including members of the client’s household, friends who regularly visit, and exposed medical staff, typically get a culture taken and are given a standard dose of penicillin G benzathine or oral erythromycin.Finally, clients under 7 are recommended to get the DTaP vaccination and clients over 7 are recommended to get the Tdap.
Both prevent diphtheria, tetanus and pertussis, but the difference is that DTaP vaccine works at full capacity against all three diseases, hence the 3 uppercase letters; while the Tdap only contains a full strength dose against tetanus, and sufficient doses for continued immunity against diphtheria and pertussis, hence the uppercase T and the lowercase d and p in the name.
Booster shots are recommended every 10 years. Alright, let’s look at the nursing care you’ll be providing for a client with diphtheria.
Management of care7:21–9:27
Your priority nursing goals are to prevent the spread of infection, promote respiratory function and oxygenation, and monitor for complications.First, place your client on droplet and contact precautions and don appropriate personal protective equipment, including mask, gloves, gown, and eye protection.
Then, start your assessment by gathering an accurate medical history, including immunization status and if they have been in contact with someone with similar symptoms.
Lastly, since diphtheria is a reportable disease, ensure you report the client’s case to your local health department.Next, focus your care on promoting respiratory function and oxygenation.
Closely monitor your client’s temperature and administer antipyretics to control fever to decrease oxygen consumption. Also encourage them to take deep breaths to promote lung expansion.
Regularly monitor their respiratory rate and effort, breath sounds, blood oxygen saturation, and mental status. Provide suction and humidified oxygen as needed.
Report to the health care provider increased respiratory rate or effort, stridor, blood oxygen saturation below 90%, or altered mental status immediately and prepare to assist with endotracheal tube placement or cricothyrotomy, as indicated.
Finally, watch closely for complications that may develop. Institute ECG monitoring, administer the prescribed IV fluids, and insert an indwelling urinary catheter.
Report any complications to the healthcare provider. For cardiac complications, report abnormal ECG or cardiac enzymes; for kidney complications, report oliguria; and finally, for neurological complications, report ptosis or double vision.
General client and family teaching9:27–10:43
Let’s move on to client and family teaching. First, explain to your client that diphtheria is an illness caused by toxins, from bacteria, that most often affects the upper respiratory tract.
Then, provide education on infection control techniques, including hand hygiene and cough etiquette, to prevent the spread of diphtheria to others.
Advise them that they will have follow-up cultures to determine when the infection has cleared, and remind them that they should remain isolated from others until two consecutive negative cultures have been taken at least 24 hours apart.
Next, remind them that their close contacts will need treatment too. By obtaining cultures, providing them with antibiotics, and ensuring everyone’s immunization status is current.Also let them know that their diphtheria infection does not result in immunity from future infections, so urge them to receive a diphtheria vaccination after their infection has cleared.Finally, teach them symptoms to watch for that could indicate complications, and instruct them to contact their healthcare provider immediately if they experience difficulty breathing, heart palpitations, and neurological symptoms like blurred vision.Alright, as a quick recap… Diphtheria is a toxin-mediated bacterial infection that most often affects the upper respiratory tract.
Review10:43–12:16
Risk factors for contracting diphtheria include being immunodeficient or unvaccinated, and coming into contact with an infected person.
Clinical manifestations usually begin with a low-grade fever, malaise, and weakness, followed by a gray pharyngeal pseudomembrane that can obstruct the airway and cause dyspnea and stridor.
A barking cough and hoarseness are also often present. Diagnosis begins with the client’s history and physical assessment, and is confirmed with cultures of swabs from the pharynx.
Treatment relies on antibiotics, and airway management through early intubation and oxygen supplementation. Vaccination can help prevent the disease.
Clients under 7 are recommended to get the DTaP vaccination and clients over 7 are recommended to get the Tdap, with booster shots recommended every 10 years.
Priority nursing goals are to prevent the spread of infection, promote respiratory function and oxygenation, and monitor for complications.
Client and family education centers on explaining what diphtheria is and its risk factors, describing home care and how to monitor for complications, preventing the spread of infection, and emphasizing vaccination to prevent reinfection.
| DIPHTHERIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below