Cardiomyopathy: Nursing
Notes
| CARDIOMYOPATHY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
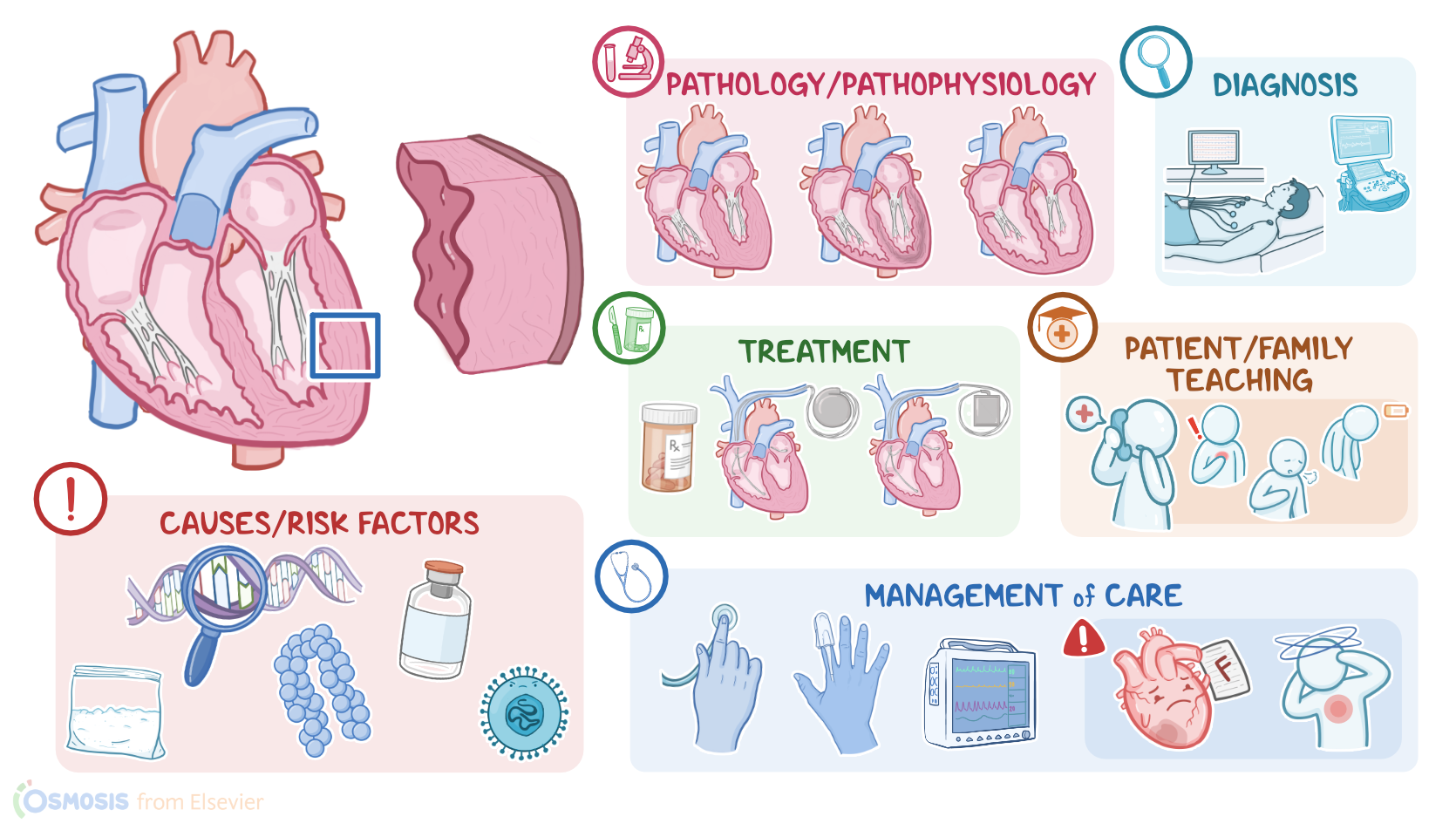
Cardiomyopathies are a group of diseases of the myocardium, which is the muscle layer of the heart wall. The three main types are dilated cardiomyopathy, which is the most common one; as well as hypertrophic, and restrictive cardiomyopathy.
Now, let’s quickly review some anatomy and physiology. The heart wall is made of three layers: the outer layer is the epicardium; the middle and thickest layer is the myocardium, which contracts in a rhythmic way to pump blood; and the inner layer is the endocardium. These layers line the four heart chambers, so the two atria and two ventricles, which are separated by the heart valves at the end of each chamber. First, there are two atrioventricular valves, the mitral or bicuspid valve on the left, and the tricuspid valve on the right. The atrioventricular valves prevent blood from returning to the atria after filling the ventricles. And second, there are two semilunar valves called the aortic valve at the left, and the pulmonary valve at the right. The semilunar valves prevent blood from returning to the ventricles after being pumped out.
Okay, when it comes to the causes of dilated cardiomyopathy, there are many potential causes, which include genetic mutations; cardiotoxic agents, such as alcohol, cocaine, lead, as well as chemotherapeutic medications like doxorubicin and trastuzumab. Dilated cardiomyopathy can also be caused by infections such as human herpesvirus 6, cytomegalovirus, or Lyme disease; nutritional deficiencies, like lack of thiamine; and metabolic disorders, like hyperthyroidism. Sometimes, dilated cardiomyopathy can also be related to pregnancy, called peripartum cardiomyopathy.
Next up is hypertrophic cardiomyopathy, which is most commonly caused by mutations in genes coding for components of the cardiac muscle cells. These mutations are typically inherited in an autosomal dominant fashion. On a side note, it’s important to distinguish hypertrophic cardiomyopathy from “athlete’s heart”, which refers to benign left ventricular hypertrophy in professional athletes.
Lastly, restrictive cardiomyopathy can be idiopathic, or it can be due to toxic; genetic; infiltrative or inflammatory causes. Some conditions that can cause restrictive cardiomyopathy include amyloidosis or hemochromatosis, where misfolded amyloid proteins, or excess iron, respectively, end up depositing in the myocardium. Other causes include sarcoidosis, as well as medications like hydroxychloroquine, and radiation therapy.
Now, let’s look at the pathology of each type of cardiomyopathy. With dilated cardiomyopathy, there’s an enlarged left ventricle chamber. As a result, the dilated heart muscle becomes really weak, so its ability to contract and pump blood becomes significantly impaired. On the flip side, in hypertrophic cardiomyopathy, the heart wall gets thicker, stiffer, and less compliant, which reduces the chamber size and ability to stretch. This most frequently affects the left ventricle, impairing the heart’s ability to fill up with blood, so less blood is pumped out with each contraction.
Additionally, the interventricular septum is also often thickened, which can obstruct blood flow from the left ventricle into the aorta, causing obstructive hypertrophic cardiomyopathy. Additionally, the mitral valve, found between the left atrium and the left ventricle, also moves abnormally, meaning that during ventricular contraction, it moves slightly forward. This further impairs adequate blood flow through the left ventricle.
Finally, with restrictive cardiomyopathy, the heart muscle becomes stiffer and less compliant. Now, the heart wall and chambers generally stay about the same size or get slightly enlarged. However, when blood fills into restricted ventricles, they can’t expand, so this again impairs the heart’s ability to fill up with blood and less blood is pumped out with each contraction.
Regardless of the type of cardiomyopathy, clients with a poorly functioning myocardium are more prone to develop several complications. First off, blood that’s not efficiently pumped out becomes stagnant in the heart, which can increase the risk of clot formation. This clot can then dislodge, and travel into the systemic circulation, and potentially to the brain, cutting off blood supply, and causing a stroke. The abnormal myocardium may also impair the function of the heart valves, ultimately leading to valvular heart disease.
Over time, as cardiomyopathy progresses, the client may develop heart failure, where the heart becomes unable to pump enough blood to meet the body’s requirements. Lastly, because cardiomyopathies affect the cardiac muscle as well as the pacemaker cells that run through the cardiac muscle, they can cause arrhythmias like atrial fibrillation, and even cardiac arrest and sudden cardiac death. In fact, hypertrophic obstructive cardiomyopathy is the most common cause of sudden cardiac death in clients less than 35 years old, and is especially more common in athletes.
Alright, now, regarding clinical manifestations, in all three types of cardiomyopathy, clients are typically asymptomatic at first. Over time, as heart failure develops, clients may experience fatigue, nausea, vomiting, and anorexia, as well as signs of left sided heart failure, like dyspnea, particularly when lying flat; fatigue and exercise intolerance; and signs of right sided heart failure, like jugular venous distention, swelling of the feet, abdominal bloating, ascites, and hepatomegaly. And because cardiomyopathies can lead to arrhythmias, clients may experience palpitations. Clients with hypertrophic obstructive cardiomyopathy can also present with syncope, which is a transient loss of consciousness; and sometimes, the presentation of hypertrophic cardiomyopathy can be sudden cardiac death.
Now, during auscultation of the heart, dilated and restrictive cardiomyopathies cause an S3 heart sound, which is the result of blood rushing and slamming into the dilated ventricular wall during diastole. On the other hand, hypertrophic cardiomyopathy produces an S4 sound in the apex of the heart. This sound indicates that the atrium is contracting against a thickened left ventricle. If there’s also valvular heart disease, heart murmurs might also be found.
The diagnosis of cardiomyopathy starts with the client's history and physical assessment, followed by an echocardiogram, which makes it possible to measure the thickness of the heart wall and dimensions of the heart chambers, as well as cardiac output, meaning how much blood the heart pumps out with each stroke. An ECG should be also performed to look for arrhythmias. In some cases, an exercise stress test might be done, to assess the heart’s ability to perform under stress. Finally, additional diagnostic tests can be also helpful, including a chest X-ray, cardiac CT and MRI scans, to visualize the heart’s shape and size, genetic testing, to look for associated gene mutations, as well as cardiac catheterization, which is used to evaluate the extent of the disease.
The goal of treatment in cardiomyopathies is aimed at symptom relief and ensuring that the heart continues to function. This involves treating the associated heart failure, and arrhythmias with medications like beta blockers and ACE inhibitors, as well as vasodilators, such as dobutamine, and milrinone, which help decrease the heart’s workload, and diuretics to reduce fluid overload. Anticoagulants can also be administered to prevent thrombus formation. Additionally, clients prone to arrhythmias need an implanted pacemaker or a cardioverter-defibrillator device or ICD. Some clients also need a left ventricular assist device or an LVAD, which is a mechanical pump that assists the heart in distributing blood. In extreme cases, a client with cardiomyopathy might require a heart transplant.
Now, some clients may require additional treatment, which depends on the type of cardiomyopathy. So, those with hypertrophic cardiomyopathy might require procedures to reduce the wall thickness, such as alcohol septal ablation, or ventriculomyotomy, and septal myectomy, where a part of the thickened septal wall is removed. For clients with restrictive cardiomyopathy, cessation of high-intensity exercise is recommended to avoid sudden cardiac death.
Alright, now let’s look at the nursing care you’ll provide for a client with hypertrophic cardiomyopathy and heart failure. Your priority goals of care are focused on improving cardiac output and managing symptoms.
Begin by assessing your client’s baseline weight, vital signs, and lung and heart sounds. Institute continuous pulse oximetry, and keep the SpO2 above 95%; and cardiac monitoring, making note of their current rhythm. Report signs and symptoms of worsening heart failure, including chest pain, pulmonary crackles, dyspnea, decreased SpO2, or tachypnea. Provide high flow supplemental oxygen and place your client in a high Fowler position. Then administer the prescribed medications to slow the heart rate, increase ventricular filling, and cardiac output; as well as medications to promote diuresis and decrease cardiac workload. Prepare to assist with catheter placement for monitoring of pulmonary and arterial pressures.