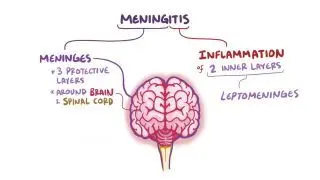
Signs and symptoms of basilar skull fractures are related to the close proximity of the skull base to cranial nerves; blood vessels; and meninges, which are the protective membranes that surround the brain and spinal cord and contain the cerebrospinal fluid (CSF). Skull base fractures increase the risk of developing meningitis because of the possible contact of bacteria in the nose, throat, or ear with the central nervous system.
Based on their location, skull base fractures can be divided into those affecting the anterior, middle, or posterior fossa. Anterior basilar skull fractures are associated with the “racoon eyes” sign, which refers to consequent bruising around the eyes. Additionally, these fractures can cause CSF to leak out through the ears or nose, resulting in the classic “halo” sign. This sign appears when CSF mixes with blood on an absorbent surface, such as paper or bed sheets, and creates a double ring pattern. Other signs of anterior basilar skull fractures include partial or total loss of vision and smell as well as eye movement defects due to cranial nerve damage.
Middle skull base fractures are the most common type and mainly affect the temporal bone and inner ear. They are associated with damage to the carotid artery as well as with hearing loss and loss of balance. These types of fractures can lead to blood pooling behind the eardrum, causing it to appear purple. Additionally, they can result in bruising behind the ear, known as the Battle sign.
Finally, posterior skull base fractures are associated with
cervical spine injury,
vertebral artery injury, and damage to the lower cranial nerves. These fractures are less common than the other two but carry the risk of damaging the
brainstem, which could be fatal.