
Anorectal Manometry. www.hopkinsmedicine.org. Published April 19, 2022. Accessed March 19, 2024. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/anorectal-manometry#:~:text=What%20is%20anorectal%20manometry%3F
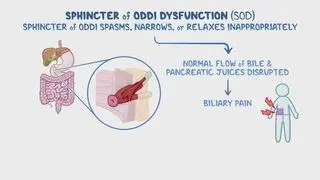
Cheon YK. How to interpret a functional or motility test - Sphincter of oddi manometry. J Neurogastroenterol Motil. 2012 Apr;18(2):211-7. doi: 10.5056/jnm.2012.18.2.211. Epub 2012 Apr 9. PMID: 22523732; PMCID: PMC3325308.
Hogan WJ. Diagnosis and treatment of sphincter of oddi dysfunction. Gastroenterol Hepatol (NY). 2007 Jan;3(1):31-5. PMID: 21960774; PMCID: PMC3096116.
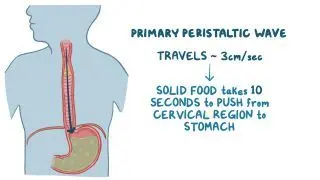
Mascarenhas A, Mendo R, O'Neill C, Franco AR, Mendes R, Simão I, Rodrigues JP. Current approach to dysphagia: A review focusing on esophageal motility disorders and their treatment. GE Port J Gastroenterol. 2023 Mar 8;30(6):403-413. doi: 10.1159/000529428. PMID: 38476159; PMCID: PMC10928869.