Assessment of gestational age: Nursing
1,376views
Notes
| ASSESSMENT OF GESTATIONAL AGE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PRENATAL |
| |
| POSTNATAL |
| |
| NEUROMUSCULAR MATURITY |
| |
| PHYSICAL MATURITY |
| |
| NEW BALLARD SCORE SYSTEM |
| |
Transcript
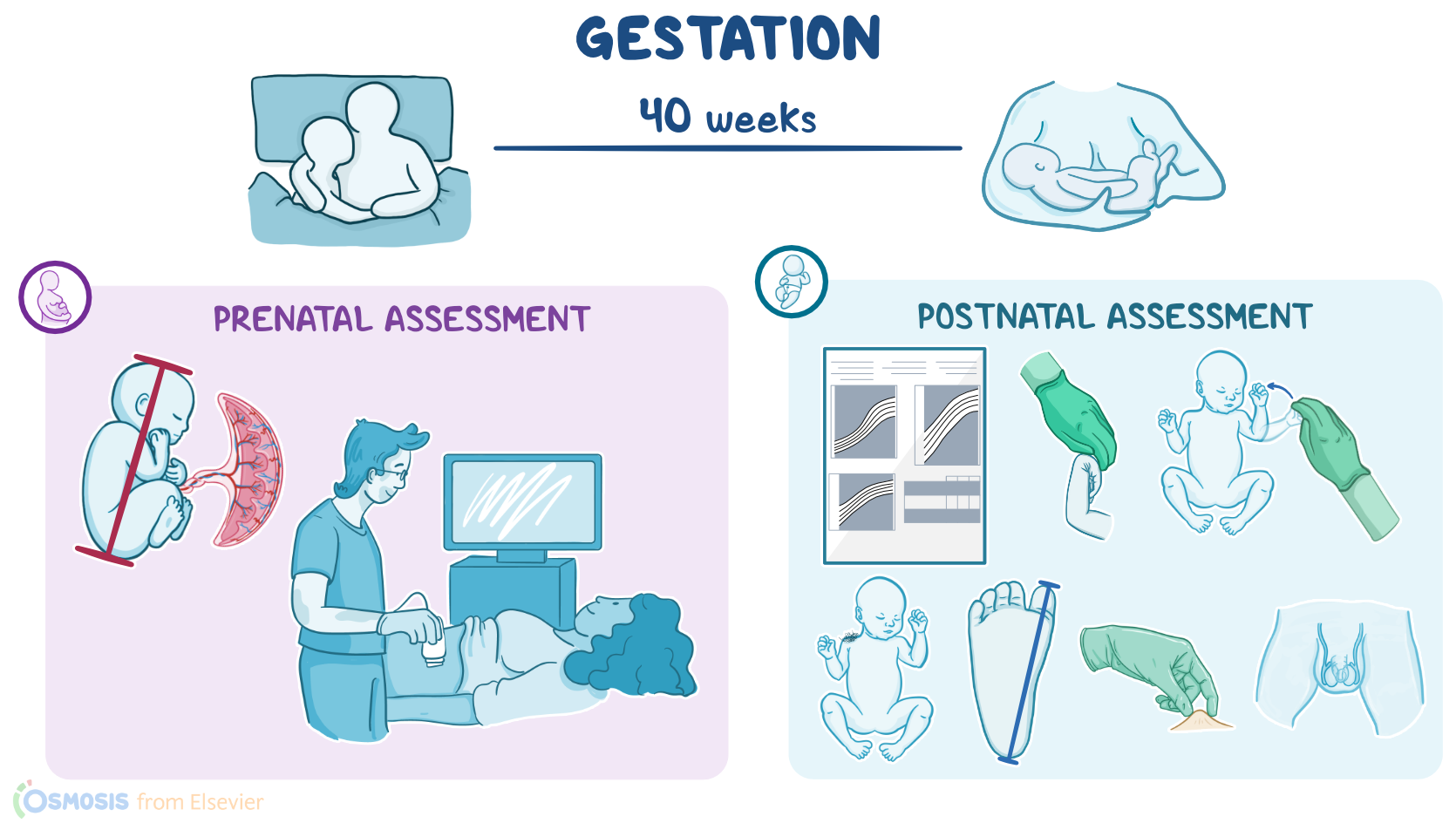
Gestation refers to the period between conception and birth, which typically lasts for 40 weeks. On the other hand, gestational age is a term used to describe a newborn based on their physical and neuromuscular characteristics. An accurate gestational age is obtained in order to provide the basis for planning care, both prenatally, meaning before birth; or postnatally meaning after birth.
First, let’s focus on prenatal assessment of gestational age, which is typically determined by the length of pregnancy after the first day of the mother’s last menstrual period, expressed in weeks and days. A much more accurate way to estimate gestational age is to use ultrasound to evaluate the size of the embryo or fetus by measuring the crown rump length or CRL for short. The CRL refers to the distance from the top of the head, or crown, down to the bottom of the buttocks, or rump. An ultrasound can be also used to measure the size of specific fetal parts, such as the cranium, abdomen, and long bones.
On the other hand, postnatal assessment is primarily determined using a scoring system called the New Ballard Score. The New Ballard Score assesses the infant’s maturity by evaluating neuromuscular and physical characteristics, where the scores for each characteristic can range from -1 to 5. Higher scores indicate a more mature gestational age, and lower scores indicate a less mature gestational age. In general, the gestational age assessment is most accurate if done within the first 48 hours after birth.
Alright, there are 6 components of neuromuscular maturity, which include posture, square window, arm recoil, popliteal angle, scarf sign, and heel to ear. Let’s start with posture, which looks at the amount of flexion of the arms, knees, and hips, as well as the degree of hip adduction or abduction. The healthcare provider places the infant in the supine position, and observes the posture when the infant is quiet and comfortable. More mature infants have a normal muscle tone and have a flexed, frog-like position. On the other hand, less mature infants typically have an abnormal muscle tone, so they tend to remain flat on the bed with their extremities limp and extended.
The second component is the square window, which assesses the flexibility of the wrist. The healthcare provider applies pressure to the dorsal side of the hand, close to the fingers, noting the angle between the infant’s palm and forearm. The angle will decrease as gestational age increases, so the palm of mature infants can even fold against the forearm, closing the angle at 0 degrees. On the other hand, less mature infants have less flexibility at the wrist, causing the angle to be greater, up to 90 degrees; and as a result, the infant’s forearm, palm, and fingers look like a square window.
Next up is the arm recoil, which evaluates the flexor tone of the biceps muscle and the strength of recoil. The healthcare provider flexes the arm at the elbows for 5 seconds. After 5 seconds, they momentarily pull down the infant’s forearms and release them, noting the angle between the forearm and upper arm, as well as the strength of recoil. The angle decreases and the briskness of recoil increases with gestational age, so more mature infants can have a brisk recoil to 90 degrees. On the other hand, less mature infants typically have a slow, partial recoil or no recoil at all.
Moving on to the popliteal angle, which evaluates the tone around the knee joint. Here, the healthcare provider holds the infant’s thigh in knee–chest position. Next, while holding the thigh in place they gently extend the lower leg and foot until they feel the resistance. The score is based on the angle between the infant’s lower and upper leg. The angle will decrease as gestational age increases, so mature infants can have a popliteal angle of 90 degrees; while less mature infants can extend their lower leg up to 180 degrees.
Now, the scarf sign evaluates the passive tone of the flexor muscles around the shoulder. The healthcare provider grasps the infant’s arm and gently pulls it across the chest, towards the opposite shoulder, and around the neck. The score is based on the position of the infant’s elbow in relation to the midline of the body. More mature infants demonstrate greater resistance, preventing the elbow from reaching the chest midline. On the flip side, less mature infants show less resistance, so their arm is easily pulled across the chest and around the neck, like a scarf.
The last neuromuscular component is called the heel to ear, which evaluates the passive flexor tone surrounding the pelvis. While keeping the infant's hips flat on the bed, the healthcare provider grasps the infant’s foot, pulling it towards the ear on the same side of the body until they feel the resistance. The distance between the foot and the ear, along with the amount of knee extension is noted. More mature infants demonstrate more flexion and increased resistance, while in less mature infants, the heel can reach closer to the ear.
Now, let’s switch our focus to the 6 components of physical maturity, which include the skin, lanugo, plantar surface, breast, eye and ear, and external genitalia. First, let’s start with the skin, which involves assessing the skin’s texture and degree of opacity. As gestational age increases, the skin thickens and transparency decreases as more subcutaneous tissue develops. If gestation progresses beyond 38 weeks, though, the skin can start to wrinkle and crack.