Biliary atresia: Nursing
Biliary atresia: Nursing
Acute Final
Acute Final
Notes
| BILIARY ATRESIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Contributors
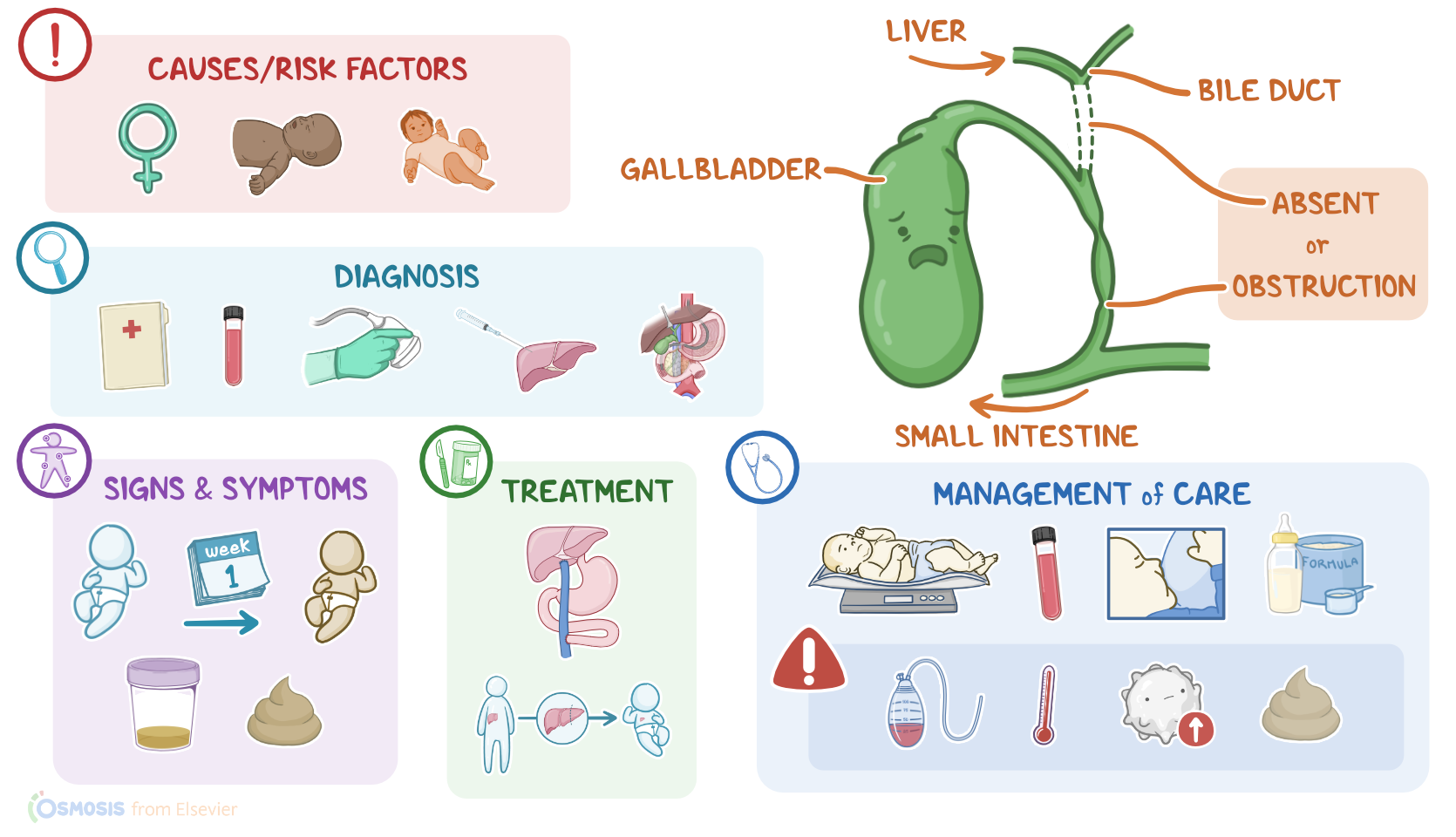
Biliary atresia refers to the obstruction or total absence of bile ducts, which results in an impaired bile flow from the liver into the gallbladder and small intestine.
Let’s start with some basic anatomy and physiology of the liver and gallbladder. Liver cells produce bile, which helps digest fats in the intestines.
The bile flows from the liver into the right and left hepatic ducts which merge to form the common hepatic duct. The common hepatic duct is where the cystic duct opens. The cystic duct functions like a two way street, allowing the passage of bile from the liver to the gallbladder, where it’s stored in between meals; while at the same time allowing bile to pass from the gallbladder, into the common bile duct, which is the part of the bile duct below the opening of the cystic duct.
Remember that the gallbladder, is a pear-shaped hollow organ found beneath the liver that stores and concentrates the bile.
So, after a high-fat meal, the gallbladder contracts and pushes the bile through the cystic duct, down the common bile duct, and into the duodenum, to help with digestion.
Afterwards, some of the bile is excreted through feces, giving them their characteristic color, while some is reabsorbed into the blood and then eliminated through urine.
Now, the exact cause of the biliary atresia is still unknown. Some theories suggest that genetic mutations can result in the abnormal fetal development of the biliary system; while others propose that biliary atresia results from some sort of inflammation of the bile ducts. The ultimate cause of this inflammation is not fully known, but it’s thought to occur because of perinatal exposure to viruses or toxic substances. This inflammation causes destruction of the bile ducts, eventually impairing bile flow from the liver.
No matter what the cause is, important risk factors that have been associated with biliary atresia include being assigned female at birth, as well as black or Asian race.
Next, let’s look at the pathology of biliary atresia. The obstruction or total absence of bile ducts results in cholestasis or impaired bile flow.
As bile starts to build up within the biliary tree, pressure in the ducts increases and the bile will eventually push its way through the tight junctions between epithelial cells lining the ducts and leak out into the blood.
A key component of bile is bilirubin, and specifically, conjugated bilirubin, also called direct bilirubin. This increases the amount of conjugated bilirubin in the blood which causes jaundice, or yellowing of skin and eyes.
At the same time, excess bilirubin makes its way into urine, and no bile gets to the intestines, which impairs absorption of fats and fat soluble vitamins, and causes pale stools.
Over time, the accumulation of bile in the liver can result in cirrhosis or even liver failure. Furthermore, since there’s no bile in the intestines, normal absorption of fat is affected and this can cause malnutrition in newborns.
In addition, other congenital defects are often present in neonates with biliary atresia. These include esophageal or intestinal atresia, intestinal malrotation, umbilical and inguinal hernias, renal anomalies, congenital heart defects, and situs inversus which is a condition where the position of the major organs are inverted, so the heart is on the right side of the body and the liver on the left side.
Clinically, newborns with biliary atresia appear normal at birth and pass normal stools. After the first week of life, they develop jaundice, or yellowing of the skin, mucosa, and eyes. As direct bilirubin increases, the infant’s skin can take on a greenish bronze color Additionally, there can be dark urine and pale stools. Finally, with biliary atresia can develop portal hypertension hepatomegaly,abdominal pain, ascites, and nausea.
The diagnosis of biliary atresia starts with the client’s history and physical assessment, followed by laboratory testing. This typically reveals elevated levels of conjugated bilirubin, aspartate aminotransferase or AST, alanine aminotransferase or ALT, and gamma-glutamyltransferase or GGT.
Imaging tests can also be used to assess the biliary system and visualize the site of obstruction, including abdominal ultrasound, endoscopic retrograde cholangiopancreatography, or ERCP; as well as percutaneous transhepatic cholangiography, and hepatobiliary or HIDA scan.
Diagnosis can be confirmed with a liver biopsy, which reveals enlarged portal tracks with fibrosis and bile duct proliferation. If the diagnosis remains unclear, an exploratory laparoscopy can be done to directly enter the abdominal cavity and inspect the condition of internal organs.
Finally, treatment includes a surgical procedure called hepatoportoenterostomy, which is often referred to as the Kasai procedure.
With the Kasai procedure, damaged bile ducts are removed, and a loop of the newborn’s intestine is cut and used as a bridge between the liver and intestines.
Although this procedure can be effective at re-establishing bile flow, a lot of newborns continue to have slowly progressing liver disease, and will often need a liver transplant.
Okay, now let’s look at the nursing care you will provide for a client with biliary atresia.
Your priority nursing goals are to provide supportive care before and after surgery, promote nutrition, and provide emotional support.