Clubfoot: Nursing
Notes
| CLUBFOOT | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Clubfoot, also called talipes equinovarus, is a complex congenital deformity that involves the ankle and foot. Let’s start by looking at the anatomy and physiology of the newborn’s foot. The foot is essential for stability, locomotion, balance and development of motor skills, so it’s important that the structures comprising the foot are well-developed. There are 3 regions of the newborn foot: hindfoot, also called rearfoot; midfoot; and forefoot. The hindfoot includes two bones: the talus and calcaneus. The midfoot includes the navicular bone, the cuboid bone and the cuneiform bones. Finally, the forefoot consists of metatarsals, which are the long foot bones; and the phalanges, which are the toe bones. Unlike the adult foot, the newborn arch is flat; has a greater range of motion and consists of more subcutaneous fat. The ankle is a synovial joint that results from interaction between the ends of the tibia and fibula, which are the bones of the lower leg, that allows the foot to move up and down.
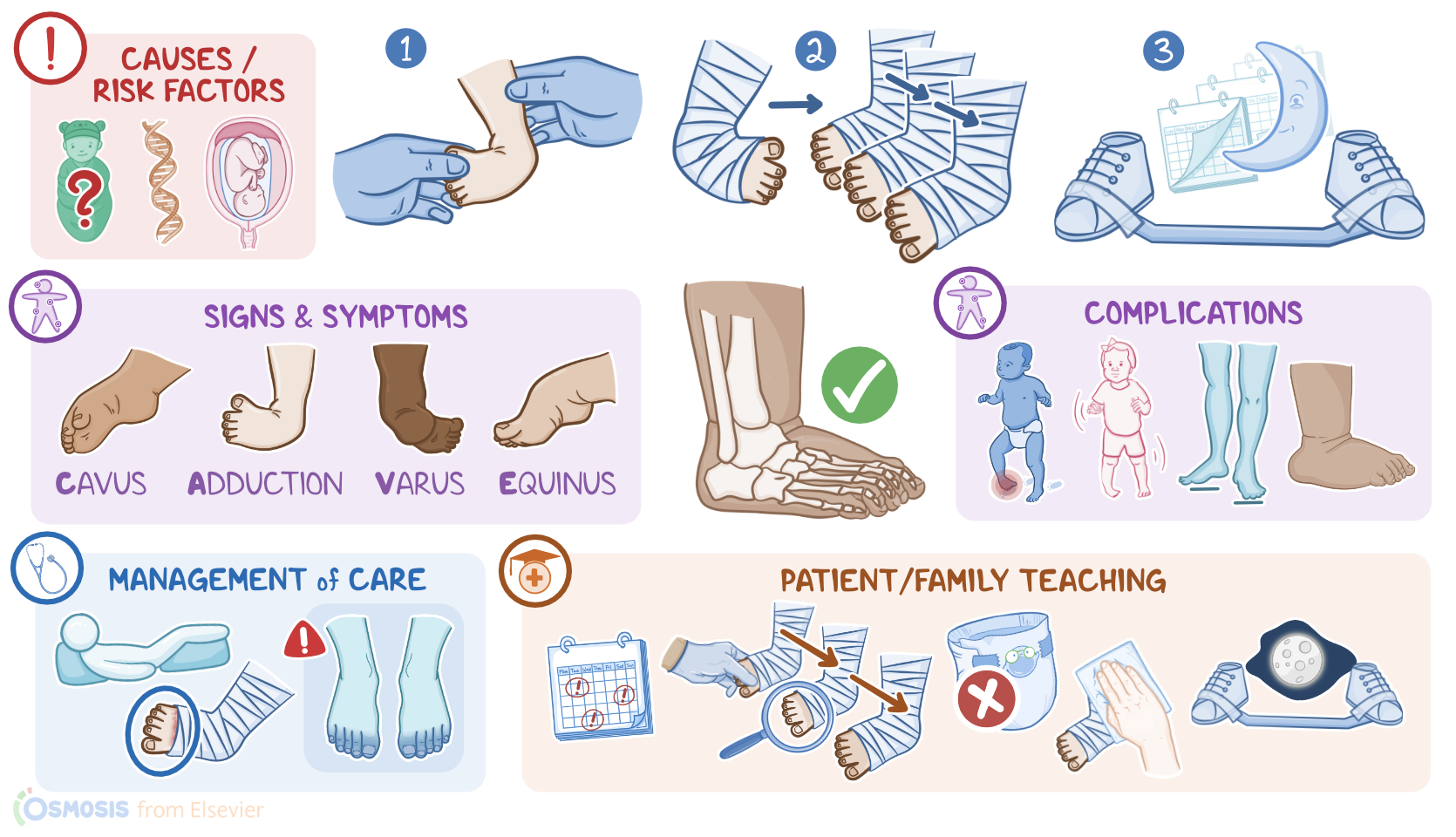
Now, the ultimate cause of clubfoot isn’t fully known, but causes can be classified as idiopathic, syndromic, or positional. If clubfoot is an isolated anomaly in an otherwise healthy neonate, it’s considered to be idiopathic. Sometimes, though, clubfoot can be syndromic, which means it’s associated with other genetic or anatomic abnormalities. Other times, the cause is positional, like with oligohydramnios, where there’s not enough amniotic fluid, or because of changes within the uterine environment that creates pressure on the fetal extremity during critical periods of development. All right, now, when it comes to pathology, clubfoot is associated with bone deformities and soft tissue contractures. There are four main components, which can be remembered by the acronym CAVE. The first one is an exaggerated arch, also known as Cavus. Second, there’s forefoot Adduction with supination, meaning that the forefoot is inverted and turned upwards.Third, inversion of the heel and hindfoot, which is called talipes Varus. Finally, there’s plantar flexion of the foot, meaning the heel is raised and the ankle is in a pointed-toe position, which is called talipes Equinus. All these components together create clubfoot, which can be unilateral or bilateral.
Left uncorrected, clubfoot can cause several complications, including inability to bear weight on the affected foot; abnormal gait; disturbances in the growth of the foot; as well as rocker-bottom foot, which is the abnormal flexion of the foot in a convex position. Clinically, varying degrees of the distinctive CAVE deformities will be noted. The flexibility of the foot will range from stiff to flexible. Now, clubfoot can be diagnosed during the antenatal period, during a routine fetal ultrasound, but usually the diagnosis is made at birth. During the neonate's physical assessment, the severity of the deformity can be scored using the Pirani system, which calculates a score based on six parameters of foot contracture; three involving the midfoot, and three involving the hindfoot. The goal of treatment is to achieve a functional, pain-free foot, so treatment should be initiated in the first two weeks of life for the best outcomes. Treatment begins with non-surgical options including manipulation to stretch the ligaments and tendons, followed by serial casting to hold the foot and ankle in the desired position. Clubfoot tends to relapse, even after it’s corrected, so after the final cast is removed bracing and corrective shoes are worn for an extended period of time.
Okay, let’s look at the nursing care you’ll provide to a child with clubfoot. Your priority nursing goals are to maintain neurovascular integrity and maintain skin integrity. After the cast has been applied, provide routine postoperative care, including assessment and management of pain. Keep a close eye on the affected foot, and do routine neurovascular checks, including color, movement, and sensation. Immediately report the presence of cyanosis, immobility, or lack of sensation to the healthcare provider. Also, be sure to check the skin around the edges of the cast, looking for areas of irritation and skin breakdown. Lastly, elevate and reposition the child’s foot routinely to decrease swelling and prevent skin breakdown. All right, let’s move on to client and family teaching. First, explain that clubfoot is a common congenital deformity involving the foot and ankle. Then, review the plan of care, and remind them to keep all their follow-up visits to ensure full correction of the deformity. Next, explain that their child’s treatment will begin with gentle manipulation to stretch the ligaments and tendons. After that, let them know that serial casting takes place over several weeks, with a new cast applied every five to seven days. While their child is in a cast, emphasize the importance of checking their child’s feet and toes often. Instruct them to observe the color and temperature of the extremity, and show them how to gently press on the toes, watch for it to lose color and then see the normal color return after pressure is released. Then, instruct them to immediately contact their child’s healthcare provider if they notice the skin turns a dark or bluish color, if there’s a loss of sensation, or if their child can't wiggle their toes.