Complete metabolic panel (CMP) - Glucose: Nursing
Complete metabolic panel (CMP) - Glucose: Nursing
NRS 42-Med/Surg-UC Davis
NRS 42-Med/Surg-UC Davis
Notes
| GLUCOSE | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
Content Reviewers
Contributors
A 63-year-old female client comes to her primary care provider’s office with reports of excessive urination and thirst; and recent weight loss despite eating and drinking more than normal. Her medical history is significant for hypertension and a BMI of 32 kg/m2. Based on the client’s assessment and medical history, the provider suspects hyperglycemia due to diabetes mellitus, and thus orders a glucose level.
Now, glucose, abbreviated as Glc, is a type of sugar that is typically obtained from consuming carbohydrates, such as bread or fruit. After a meal, glucose gets absorbed from the gut into the blood and from there it enters the cells where it is used as a source for energy.
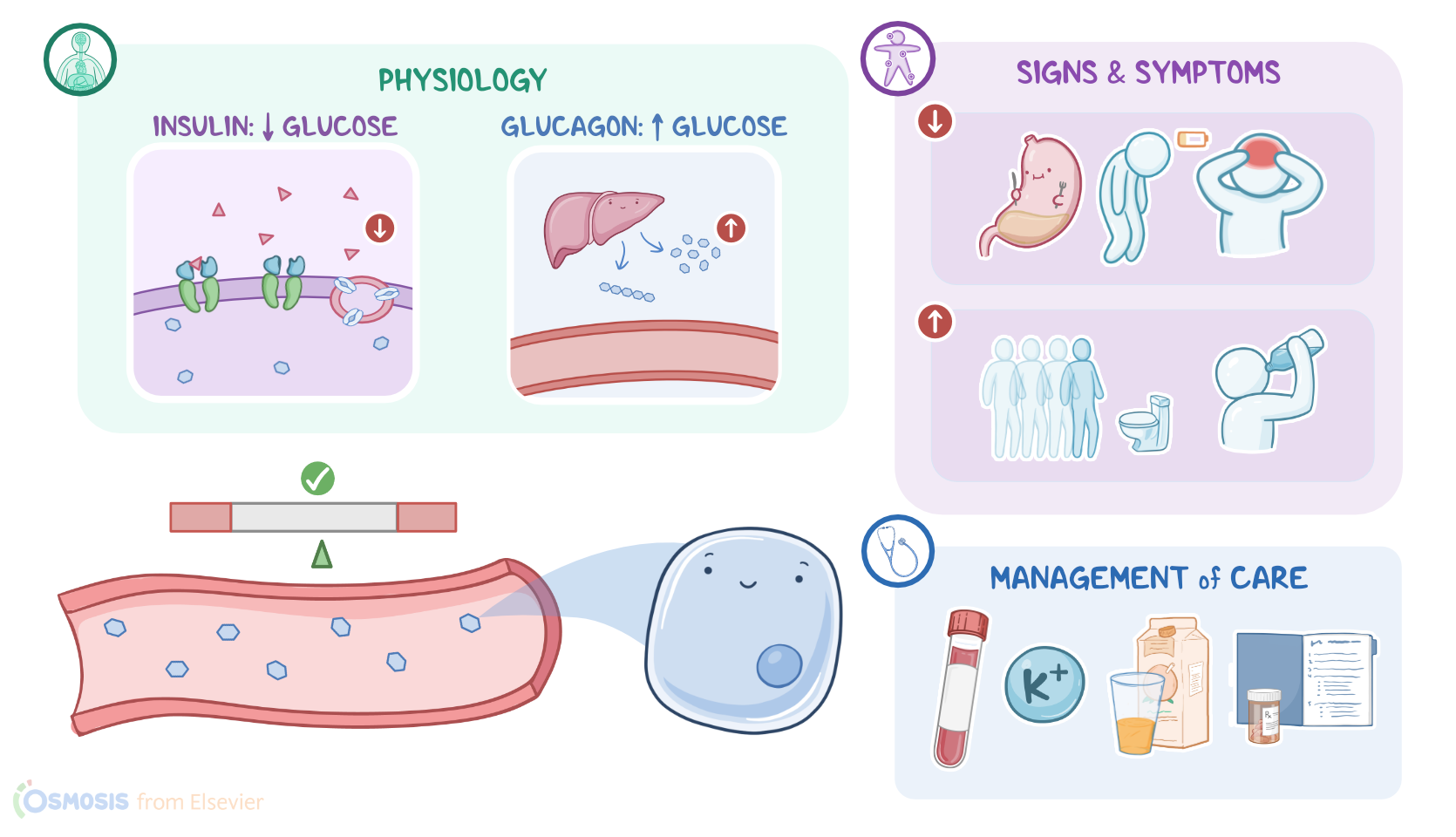
The body controls how much glucose is in the blood relative to how much gets into the cells with two hormones: insulin and glucagon. Insulin is used to reduce blood glucose levels, and glucagon is used to increase blood glucose levels.
Both of these hormones are produced by clusters of cells in the pancreas called islets of Langerhans. Insulin is secreted by beta cells in the center of the islets, and glucagon is secreted by alpha cells in the periphery of the islets.
Insulin reduces the amount of glucose in the blood by binding to insulin receptors embedded in the cell membrane of various insulin-responsive tissues like muscle cells and adipose tissue. When activated, the insulin receptors cause vesicles containing glucose transporters that are inside the cell to fuse with the cell membrane, allowing glucose to be transported into the cell. Glucagon does exactly the opposite, it raises the blood glucose levels by getting the liver to generate new molecules of glucose from other molecules and also break down glycogen into glucose so that it can all get dumped into the blood.
Plasma glucose, also referred to as blood sugar, is usually measured as part of a complete metabolic panel, or CMP, or as part of a basic metabolic panel, or BMP. It can also be measured at the point of care, or POC, by fingerstick. The normal range of plasma glucose measured after fasting, is around 70 to 99 mg/dL. However, plasma glucose can also be measured after a meal, called postprandial, to see how the body responds. This level should be less than 120 mg/dL.
The most common reason for hyperglycemia is diabetes mellitus, where the body has trouble moving glucose from the blood into the cells. This leads to high levels of glucose in the blood and not enough of it inside the cells, and remember that the cells need glucose as a source of energy, so not letting the glucose enter means that the cells starve for energy despite having glucose right on their doorstep. Generally, a level of 100 to 125 mg/dL indicates prediabetes; and 126 mg/dL or higher indicates diabetes. A non-fasting or random glucose test can be done at any time, with 200 mg/dL or higher being a red flag for diabetes. Finally, postprandial glucose of 140 mg/dL to 199 mg/dL indicates prediabetes and 200 or above indicates diabetes. Hyperglycemia may also occur in conditions such as chronic pancreatitis, Cushing syndrome, or hyperthyroidism.
Alright now classic symptoms of elevated glucose include polyuria, which means frequent urination, along with polydipsia, which means being constantly thirsty and needing to drink a lot of water. Many clients also present with polyphagia, which is a fancy way to say they have a large appetite. But, in spite of needing to eat a lot, clients experience unexplained weight loss because, since there’s no insulin, the tissue cells can’t uptake the glucose from food.
Now, clients with type 1 diabetes are at risk for a serious acute complication called diabetic ketoacidosis, or DKA for short, which presents with nausea, vomiting, dehydration, and a characteristic fruity smelling breath, as well as a deep and labored breathing called Kussmaul respirations. DKA can also cause mental status changes and even cerebral edema.
An acute complication that is much more common in type 2 diabetes is called hyperosmolar hyperglycemic state, or HHS, which is characterized by extreme hyperglycemia and polyuria which can cause severe dehydration. Nausea, vomiting, and mental status changes may also be present.
Let’s switch gears and talk about hypoglycemia, which is when blood glucose levels drop below 70 mg/dL. Hypoglycemia most often occurs in people with diabetes if they take too much insulin or certain oral antidiabetic medications, but it can also be a result of not eating enough or exercising more than usual in clients who don’t have diabetes.
Other possible causes for hypoglycemia include advanced liver disease, Addison disease, pancreatitis, and malnutrition. Finally, hypoglycemia with no clear cause may indicate the presence of a rare insulin-producing pancreatic tumor called an insulinoma.