Detached retina: Nursing
Notes
| DETACHED RETINA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Contributors
Retinal detachment occurs when the neurosensory layer of the retina is separated from the underlying retinal pigment epithelium, resulting in fluid accumulation between the two layers.
Okay, but first, a bit of physiology. The eye is made up of three major layers. There's a fibrous outer layer, which contains the cornea and sclera. The middle vascular layer is called uvea and consists of the iris, pupil, choroid, and ciliary body. Finally, the neural layer consists of the retina, with its own outer pigmented layer, and an inner neural layer that’s composed of photoreceptor cells, which convert light into neural signals that travel via the optic nerve to the brain for visual processing.
Now, there’s two kinds of photoreceptors: rods, which are great for seeing in low light conditions but only offer black and white vision; and cones, which are less sensitive but can detect different colors. So, there’s an oval spot in the middle of the posterior retina, called the macula, that has a depressed spot called the fovea at its center. The fovea contains the highest concentration of cones and is the part of the retina that offers the highest visual acuity.
Now, if we take a closer look at a cross-section of an eye, we can see that it’s split into three different chambers: anterior, posterior, and vitreous. The anterior chamber includes the area from the cornea to the iris. The posterior chamber is a really narrow space between the iris and the lens. Finally, the much larger vitreous chamber includes the space between the lens and the back of the eye. Now, both the anterior and posterior chambers are filled with a clear watery fluid called aqueous humor, while the vitreous chamber is filled with a clear but thicker fluid called vitreous humor.
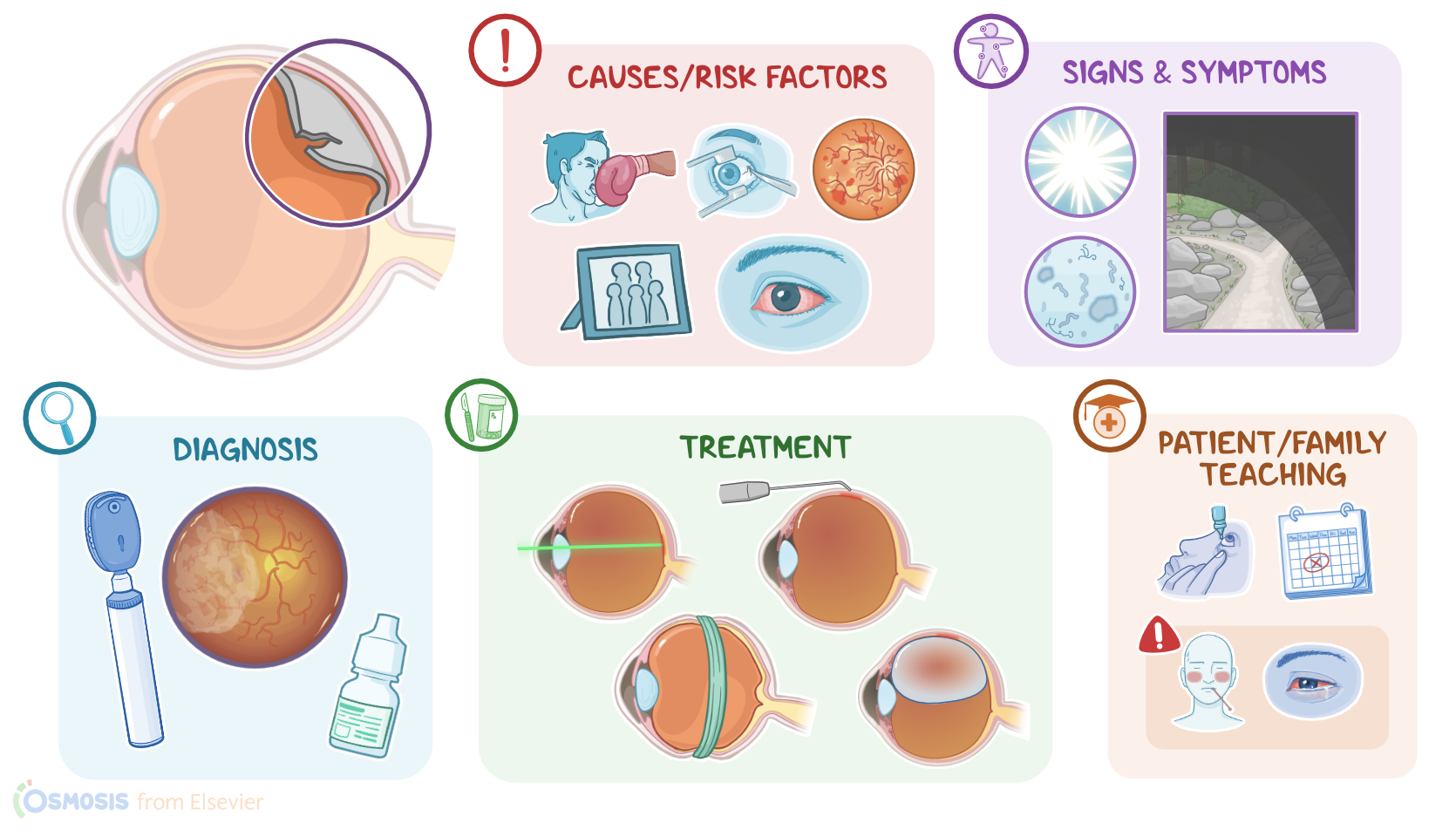
Now, the cause of retinal detachment can be rhegmatogenous or non-rhegmatogenous. The most common type is rhegmatogenous, which happens when a tear or hole causes a break in the retina, which allows vitreous fluid to move underneath the retina, causing it to separate from the back of the eye. This can be secondary to trauma to the eye, or due to the natural process that occurs with aging, where the vitreous humor changes from being a thick gel to a watery fluid. The liquefied vitreous fluid can then seep under the retina, causing it to detach.
On the other hand, non-rhegmatogenous detachment includes traction retinal detachment and exudative detachment. In traction retinal detachment, scar tissue on the retina pulls it off the back of the eye, which can happen in clients with diabetic retinopathy; while in exudative detachment, either serous or hemorrhagic fluid leaks from inflamed blood vessels and accumulates underneath the retina.
So, common risk factors for retinal detachment include advanced age, eye trauma or previous intraocular surgery, diabetic retinopathy, and family history. Retinal breaks are also much more common in clients with severe myopia, ocular inflammation or uveitis, and in those who have had a previous retinal detachment, either in the same or the contralateral eye.
Okay now, once the neurosensory retina is detached, it no longer receives nourishment from the pigmented layer and becomes ischemic. So, the part of the retina that is affected is incapable of processing light stimuli and vision is lost in that area. When this happens in the macula, visual acuity decreases significantly. If left untreated, this can progress and affect the whole retina leading to one-sided blindness.
Symptoms of retinal detachment include light flashes or floaters described as fine dots, veils, cobwebs, clouds, or strings; followed by sudden visual field loss in the affected eye. This typically begins in the periphery, and progresses toward the central visual axis over hours to weeks like a “curtain drawn down”. It’s important to keep in mind that retinal detachment is usually painless, except for cases associated with an inflammatory disorder.
Diagnosis of retinal detachment is based on the client’s history and physical assessment. This includes visual acuity testing; as well as visualizing crinkling of retinal tissue or changes in blood vessel direction by using an ophthalmoscope or a slit lamp. Mydriatic eye drops, such as tropicamide, are typically used before examination to dilate the pupil and better assess the retina.
Treatment for retinal detachment is surgical. One way retinal detachment can be sealed is by inducing the formation of scar tissue in that area, which is typically done with laser photocoagulation or cryopexy. Another way is to apply pressure so that the two layers of the retina come close together. This can be done with scleral buckling, where a circular silicone implant is placed around the sclera; or through pneumatic retinopexy, where a bubble of gas is injected into the vitreous to push the inner layer of the retina towards the outer layer.