Genital warts: Nursing
Genital warts: Nursing
Medical Surgical
Medical Surgical
Notes
| GENITAL WARTS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
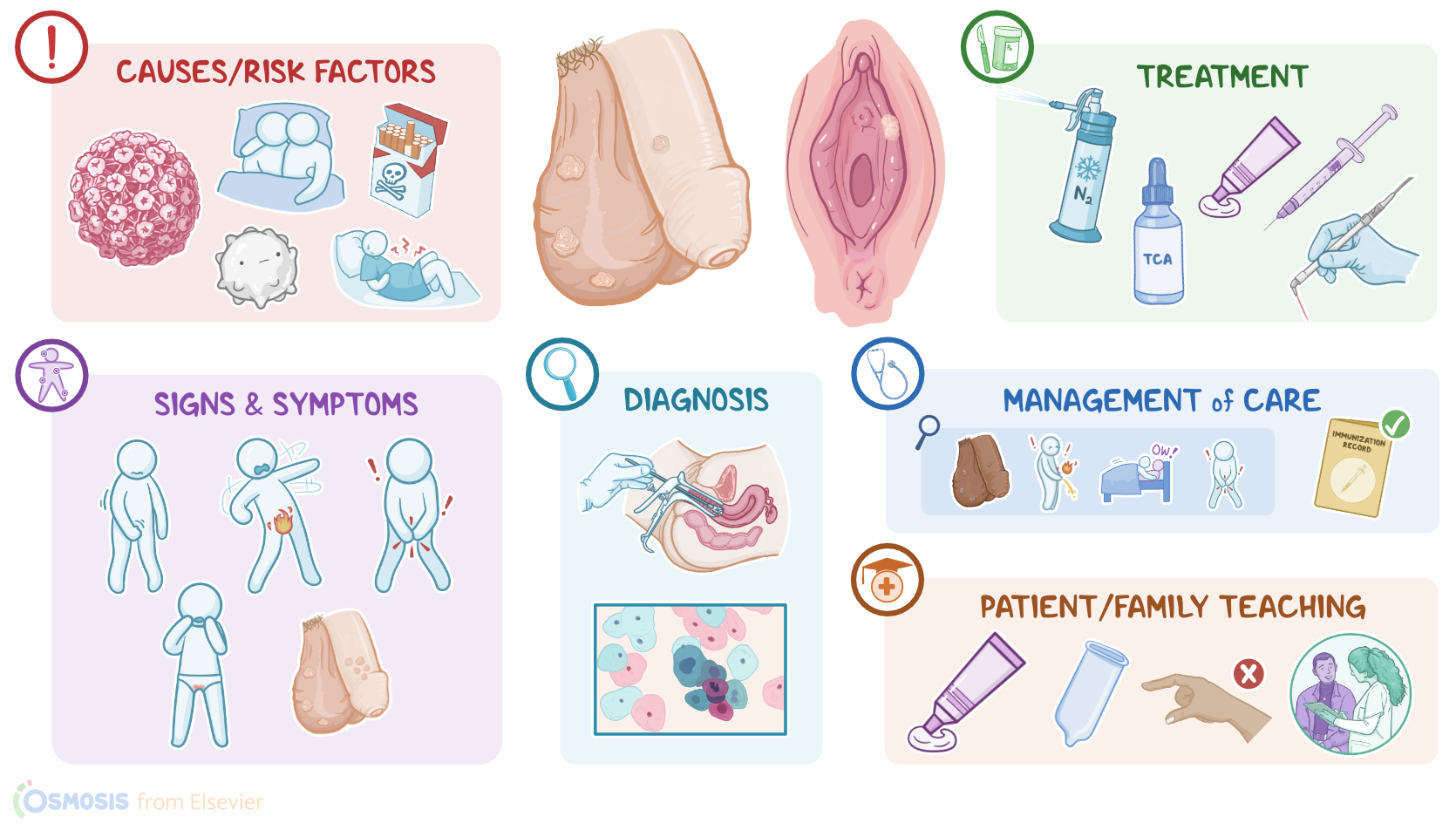
Genital warts, also known as condylomata acuminata or anogenital warts, are benign but highly contagious skin growths, typically around the genital or anal area.
Now, let’s go over some physiology. The outermost layer of the skin is called the epidermis, and it has multiple cell layers that are composed of developing epithelial cells. The innermost layer, called the basal layer, contains basal cells, which continually move up in the epidermis and divide and replicate to form new cells that replenish it. As these cells move up, they mature, become flatter, and lose their ability to replicate. Ultimately, when the cells reach the top layer, they are shed from the epithelium, so that a new generation of cells can come in and take their place.
Now, genital warts occur due to infection of the basal cells caused by human papillomavirus, or HPV for short, which is one of the most common sexually transmitted infections, or STIs. HPV is a large family of DNA viruses with over 100 strains; specifically, genital warts are most commonly caused by HPV strains 6 and 11, which are considered to be low-risk because they typically cause benign growths. On the other hand, high-risk HPV strains 16 and 18 have a high risk of causing malignant growths, including cancer of the cervix, anus, and penis, as well as cancer of the upper respiratory tract.
Now, HPV infection is typically spread through direct skin-to-skin contact with an infected client, and there is a higher risk in clients who engage in unprotected sex or who have multiple sexual partners. Additional risk factors include early age at first sexual intercourse, smoking, or having a compromised immune system. Finally, pregnant clients are at risk of transmitting HPV to their baby during labor.
Normally the basal cells are well protected underneath all the other epidermal layers. However, if there are micro-abrasions or cuts in the epidermis, HPV can gain access to the basal cells and infect them. Once that happens, HPV replicates by causing the infected cells to divide uncontrollably, thus forming these benign skin growths called warts.
Now, genital warts typically manifest as soft, flesh-colored growths that tend to have a cauliflower-like look to their surface. In some cases, these lesions may appear hyperpigmented, white, or gray. Most often, they involve the genital area, including the penis, or the vulva, vagina, and cervix, as well as around or inside the anus; clients who engage in oral sex may also develop them in the mouth or throat. Genital warts are usually painless, but they can cause itching, burning, local pain, or bleeding. If left untreated, genital warts can grow in size and multiply into clusters.
Diagnosis of genital warts involves history and physical assessment. A bright light or a dermatoscope can be used to better visualize the warts. Some clients can be assessed with colposcopy, which is when a magnifying device called a colposcope is used to examine the cervix. In some cases, a biopsy can be performed to confirm the diagnosis. Clients with genital warts should undergo regular screening tests for cervical cancer. These include performing a Pap smear, or Papanicolau test, along with HPV DNA testing to rule out the possibility of co-infection by a high-risk HPV strain.
Treatment of genital warts varies mostly depending on their size. Small warts can be treated with liquid nitrogen cryotherapy; trichloroacetic acid products; or topical immune modifiers, like imiquimod or sinecatechin, which boost the immune system’s ability to clear the infection. On the other hand, larger warts typically require laser therapy or surgery to be removed. Finally, genital warts can be prevented with vaccination. Unfortunately, most genital warts have a tendency to return even after undergoing appropriate treatment, so re-occurrences are common.
Okay, let’s look at the nursing care for a client with genital warts. Priority goals include elimination of existing warts, and providing supportive care while your client is undergoing treatment. First, assess the affected area, making note of the size and location of the warts, and assess for other signs of STIs.
Report to the healthcare provider if you notice ulcerations, vesicles, abnormal vaginal or penile discharge, or if the client lets you know they are experiencing symptoms like pain or burning with urination, pain during intercourse, and pain in the pelvic area. Lastly, confirm your client’s HPV vaccination status.