Geriatric considerations - Sensory: Nursing
Notes
| GERIATRIC CONSIDERATIONS - SENSORY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| TOUCH |
| |
| VISION |
| |
| HEARING |
| |
| TASTE AND SMELL |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
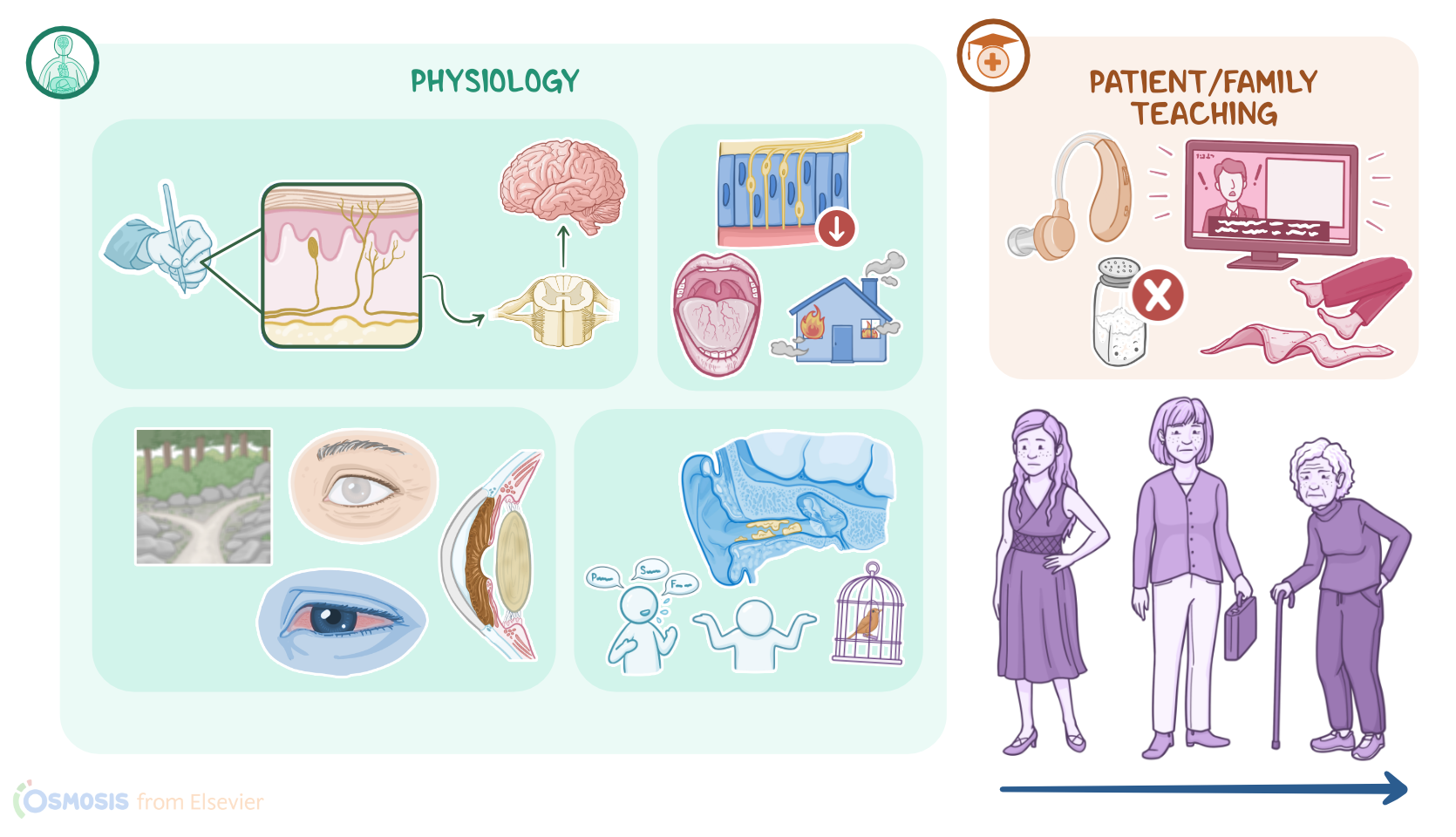
Geriatrics is the branch of healthcare dealing with both the physiology and psychology of aging, as well as the diagnosis and treatment of diseases affecting older adults. As we age, the body undergoes various changes, such as a decline in the function of the sensory system, which gathers information about our surroundings and what’s happening inside our bodies. The sensory system includes touch, vision, hearing, taste, and smell. Age-related changes in the sensory system can impact many aspects of a client’s quality of life, and thus must be taken into consideration when caring for elderly clients.
First, let’s start with touch. Tactile receptors are nerve endings that pick up sensory information when something comes in contact with your skin, like when you’re holding a pen. This sensation is then sent through sensory neurons to the spinal cord and eventually to the brain. Now, some parts of your body, like the tips of the fingers, are more sensitive to touch because they have more tactile receptors than other areas, like your back.
Now, with aging, the blood flow to nerve endings, the spinal cord, and even some parts of the brain can decrease, which causes a decreased sensation of touch. Additionally, chronic conditions, like diabetes mellitus, can affect small blood vessels that supply nerve endings and further affect sensation, particularly in distal parts of the body, like the feet. The loss of sensation makes it hard for older clients to feel pressure in specific areas of the body, which can result in complications, such as frostbites, burns, or even pressure ulcers.
Next up is vision. If we zoom into the wall of the eye, there's an outer fibrous layer made out of the cornea and sclera, which helps control and focus the entry of light. The light that passes through the cornea is directed to the lens, which in turn collects light arrays and focuses them into the retina at the back of the eye. Behind the lens is a gel-like structure called the vitreous body, which fills up the center of the eye and supports the retina. The retina is a layer that houses photoreceptors, which translate light into electrical impulses. These impulses are then carried by the optic nerve into the brain, which processes the impulses from both eyes and fuses them into one clear image.
Now, with aging, the elasticity of the lens decreases, subsequently decreasing the visual acuity and causing presbyopia, which refers to a decreased ability to focus on near objects. The cornea tends to become flattened, which can result in corneal astigmatism and symptoms such as blurry vision. Next, the quantity and quality of tear production diminishes with aging, resulting in dry eyes. Often, there is yellowing or clouding of the lens, which causes the lens to act as a filter, absorbing more blue, green, and violet light. As a result, the client might have challenges differentiating these colors.
Finally, elderly clients are at risk for developing several eye conditions, including cataracts, which are cloudy areas in the lens that reduce the sharpness of images that reach the retina; as well as glaucoma, which refers to intraocular pressure caused by blockage of the drainage of the aqueous humor; and senile miosis, meaning pupils become smaller and lose some of their ability to constrict, causing difficulties to adjust from light to dark environments.
Switching gears and moving on to hearing. The external ear is made of the auricle, also called the pinna; and the external acoustic canal, which is lined with a waxy substance called the cerumen. Cerumen prevents foreign objects, like dust or tiny insects, from getting into the ears and causing damage. At the end of the external acoustic meatus, there’s the thin, oval tympanic membrane, more commonly known as the eardrum, which separates the external ear from the middle ear. When sound waves hit the tympanic membrane, it vibrates and transfers the vibration to the middle ear, which is a tiny chamber that houses the three auditory ossicles, called the malleus, incus, and stapes. These bones create a chain that further transmits these vibrations to the inner ear, which houses the membranous labyrinth, bony labyrinth, and cochlea. Moreover, the cochlea contains small sensory hair cells that create nerve impulses that travel through the vestibulocochlear nerve, which is cranial nerve VIII, to the brain.
With aging the number of cochlear hair cells and the nerve fibers that transport electrical impulses reduces, which results in what’s known as sensorineural presbycusis. These clients usually cannot understand high-frequency sounds and conversational tones, such as F, S, and P. Other important age-related changes include the thickening of the tympanic membrane and build-up of cerumen. Furthermore, cerumen can become dry and impacted, subsequently worsening the presbycusis.
Next up is taste and smell. When you eat food or drink a beverage, your saliva acts as a solvent for different chemicals coming from what you ingested. These dissolved chemicals then stimulate taste buds, which cover the surface of the tongue. Each taste bud may contain up to one hundred chemoreceptors, which are specialized types of cells that sense, and convert chemical signals into electrical signals, which travel through sensory nerves to the brain. Similar to taste, chemicals from odors are dissolved in the mucus secreted by the nasal cavity. These chemicals then stimulate smell chemoreceptors, which are present on the roof of the nasal cavity, and get converted into electrical signals that go to the brain.