Nutrition - Enteral: Nursing skills
Notes
| NUTRITION - ENTERAL | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| FEEDING SCHEDULES |
| |
| ADMINISTERING ENTERAL FEEDINGS |
| |
| CLINICAL IMPLICATIONS |
| |
Transcript
Enteral nutrition provides fluids and nutrients directly into the GI tract through a feeding tube. As a healthcare professional, you’ll be responsible for caring for patients receiving enteral nutrition.
Now, enteral nutrition might be especially helpful for patients who have difficulty chewing or swallowing as a result of head or neck trauma; surgery; coma; dementia; nervous system disorders; or tumors of the head, neck, or esophagus.
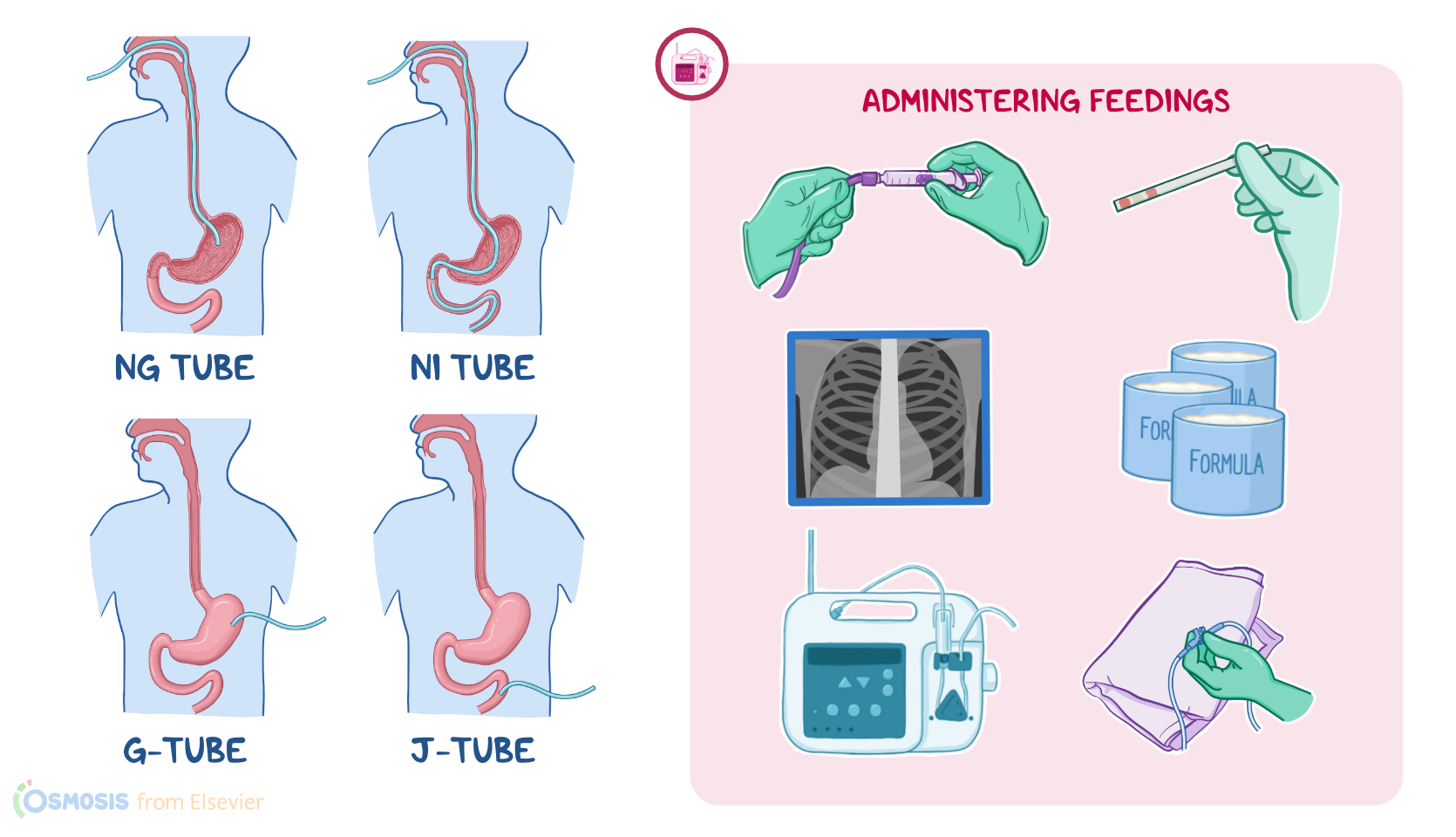
Now, there are various ways a feeding tube can go into the GI tract. The most common one is a nasogastric, or NG, tube that goes through the nose and then down into the stomach. A naso-intestinal, or NI tube, also goes through the nose, but it ends in the small intestines.
Tubes can also be inserted through a surgical opening, or stoma, in the abdominal wall and into the stomach, known as a gastrostomy tube, or G-tube. A common type of gastrostomy tube is a percutaneous endoscopic gastrostomy tube, or PEG tube for short, that’s inserted directly into the stomach percutaneously with endoscopic guidance. Finally, tubes can also be inserted into a part of the small intestine called the jejunum, known as a jejunostomy tube, or J-tube.
J-tubes, G-tubes, and PEG tubes are usually inserted if long-term tube feedings are anticipated and are typically used for more than six weeks; whereas NG and NI tubes are mostly preferred when tube feedings are needed for a short period of time, typically a few days or up to six weeks.
Once the feeding tube is inserted, its placement is confirmed by X-ray. After that, your patient can start receiving enteral nutrition through the tube. There are different types of nutritional formulas that can be ordered depending on your patient’s needs. When you first start a feeding, you’ll usually begin feeding slowly while you watch for nausea, abdominal pain, or diarrhea that could indicate feeding intolerance. If the initial rate and amount of feeding is tolerated, the feedings can be increased to the desired amount.
Now, enteral nutrition is commonly administered using an infusion pump. In this case, administration schedules can be either continuous or intermittent. A continuous feeding is when a patient has feedings running through their feeding tube throughout the day. On the flip side, if feedings are scheduled at intervals over the course of the day, this is called an intermittent feeding.
Before starting a feeding, first review the patient’s chart, collect your supplies, and make sure you have the correct formula. Identify your patient, inform them about the procedure, and answer any questions related to the procedure. Then, perform hand hygiene and apply clean gloves.
Now, keep in mind that sometimes the tip of the feeding tube can move to a different location, like from the stomach to the intestines or esophagus, or from the intestines to the stomach. So, you’ll need to verify the tube’s position before starting the feeding by checking the appearance and pH of fluid aspirated through the tube.
To do this, draw up 30 mL of air into a 60 mL enteral syringe, connect the syringe to the end of your patient’s tube and gently instill the air. Then, slowly retract the plunger and aspirate 5 to 10 mL of fluid, transfer it to a medicine cup, and observe the fluid’s appearance. Gastric fluid can range in color from clear and colorless or pale yellow or green if your patient has been fasting at least four hours. If there’s still formula in the stomach, the fluid will look like curdled milk. Intestinal fluid is often stained by bile, so color can range from golden yellow to greenish brown.
Next, test the pH by applying a few drops of fluid onto a pH indicator strip, or you can dip the strip into the medicine cup. Use a color chart to determine the pH. For gastric fluid, a pH of 0 to 4 is normal if your patient has been fasting for at least four hours; a pH 5 to 6 may occur if they’re receiving continuous feedings; and a pH more than 6 means the tube is in the esophagus, lung, or small intestines. If the pH does not match the desired location of the tube, the feeding should be held until the tube is replaced or placement is confirmed with imaging.
Once tube placement is confirmed, prepare to administer the feeding. For feedings that will run through an enteral feeding pump, you’ll use either an open or closed system. If you’re using an open system, you’ll need cans of the prescribed formula, an administration bag, and an administration set.
First, check the expiration date, then shake the cans, and cleanse the tops before opening them. Attach the tubing to the bag, clamp it to prevent the formula from running through the tube, and pour the formula into the bag.
Sources
- "Clinical nursing skills & techniques (11th ed.). ISBN 978-0-443-10718-4 " Elsevier (2025)
- "Fundamentals of nursing (12th ed.). " Elsevier (2026)
- "Alexander’s Nursing Practice: Hospital and Home. 5th edition. ISBN: 978-0-7020-6230-8 " Elsevier (2019)
- "Clinical Nursing Skills and Techniques - E-Book. 10th ed. ISBN 978032379653 " Elsevier Health Sciences (2021)
- "Fundamentals of Nursing. 11th edition. ISBN: 978-0-323-81034-0 " Elsevier (2022)
- "A guide to enteral nutrition in intensive care units: 10 expert tips for the daily practice. 25(1):424. Published 2021 Dec 14. " Crit Care (2021)
- "Krause and Mahan’s Food and the Nutrition Care Process. 16th edition. ISBN: 978-0-323-81025-8 " Elsevier Canada (2022)
- "Critical Care Nursing: Diagnosis and Management. 9th edition. ISBN: 978-0-323-64295-8 " Elsevier (2021)