Parkinson disease: Nursing process (ADPIE)
1,857views
Parkinson disease: Nursing process (ADPIE)
Watch later
Watch later
Notes
| PARKINSON DISEASE | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Michael Desante is a 67 year old male with a history of Parkinson disease. His daughter has been his primary caregiver since his diagnosis, however, as Michael’s disease progressed, Michael moved into a long-term care center for further support.
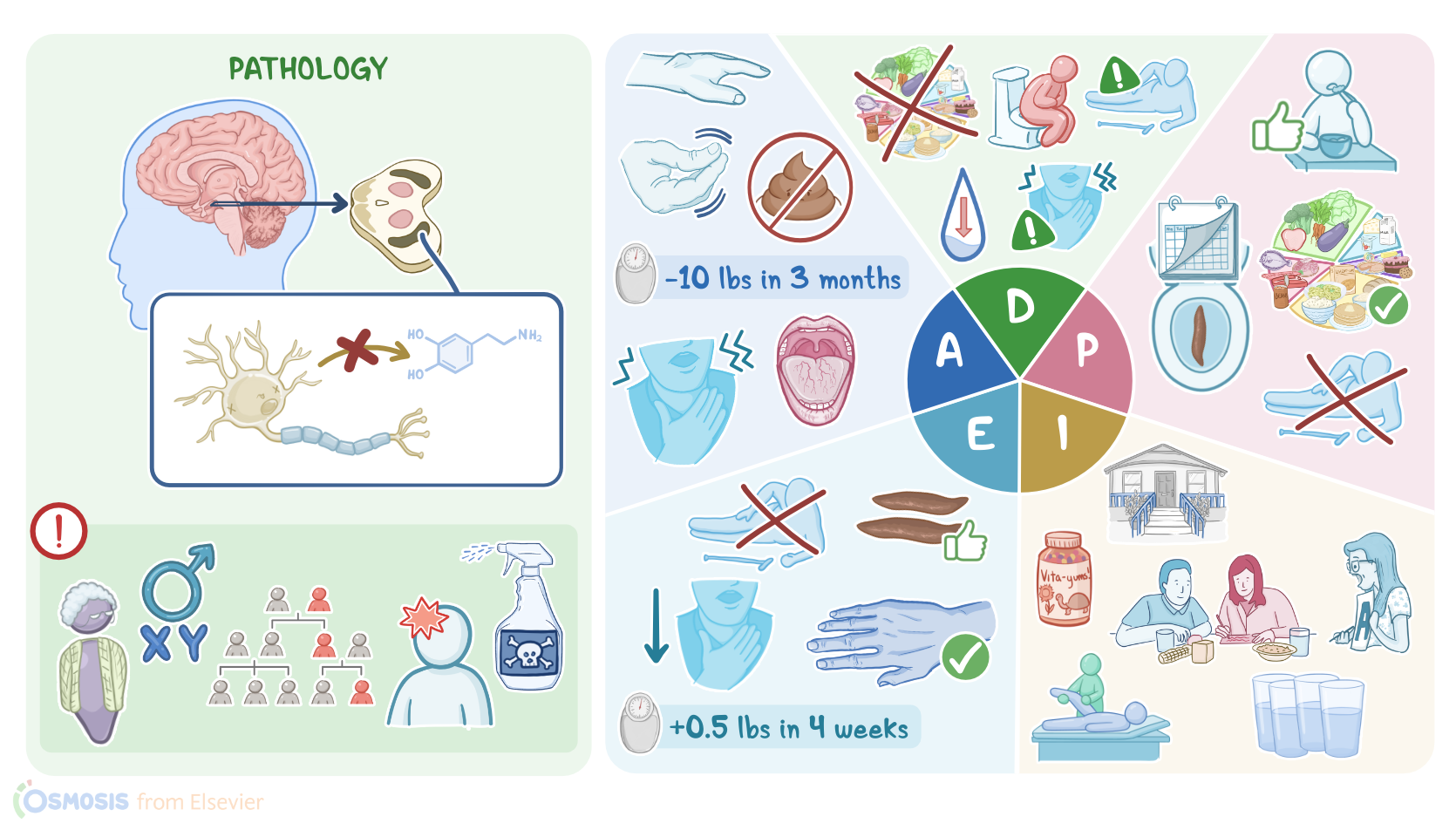
Parkinson disease, or PD for short, is a progressive neurological disease that affects movement. Most often, the cause of PD is unknown, but there are some factors that can increase the risk.
Non-modifiable risk factors include increasing age, with a mean age of onset of 57 years; as well as male sex; and having a family history of PD.
On the other hand, modifiable risk factors include exposure to toxins like pesticides, and a history of head trauma. Now, in PD there’s degeneration of the dopamine-producing neurons in the substantia nigra of the basal ganglia.
Normally, the substantia nigra helps initiate movements, but also fine tunes the way that movements happen. When these neurons die, the first symptom is a resting tremor, which is an involuntary shaking that presents at rest and decreases with movement.
Most often, resting tremor affects the hands, which is called a “pill-rolling” tremor because it looks like someone is rolling a pill between their thumb and index finger.
Over time, resting tremor can also involve the feet, tongue, and jaw. In addition, the client can experience bradykinesia, or slowness of voluntary movement.
A more severe form of bradykinesia is akinesia, which is when they become unable to initiate a voluntary movement. For instance, the client may feel like their legs freeze up when trying to walk.
Another typical symptom is “cogwheel” rigidity, which is a type of stiffness characterized by a series of catches or stalls as a person’s arms or legs are passively moved by someone else.
And because of rigidity of facial muscles, some clients with PD may have a mask-like facial expression, as well as difficulty speaking, chewing, and swallowing.
As a result, food, fluid, or saliva may enter the lungs, causing aspiration pneumonia. Decreased intake can put the client at risk for nutritional problems.
Additionally, clients may acquire a stooped posture, and a late feature of the disease is postural instability, which causes problems with maintaining balance and can lead to falls.
Now, PD can also cause non-motor symptoms, like urinary incontinence and constipation. Finally, some clients may develop sleep disturbances, apathy, depression, dementia, and an impaired sense of smell.
Okay, now diagnosis of PD mainly relies on physical examination and the presence of bradykinesia in addition to at least one of either akinesia, tremor, rigidity, or postural instability.
Ruling out other potential causes is also required. Sometimes, the diagnosis can be confirmed by administering L-dopa, which is a precursor of dopamine.
If the client’s symptoms improve, the diagnosis is confirmed. Another diagnostic test that can be used to confirm diagnosis is the DaT scan, which is an imaging technique that helps visualize the dopamine levels in the brain.
Unfortunately, there’s no cure for PD, but there are medications that can help with its symptoms by increasing the amount of dopamine in the brain. The drug combination levodopa-carbidopa is a common treatment.
Levodopa is a dopamine precursor that’s converted into dopamine in the brain, while carbidopa prevents levodopa from being broken down.
Sometimes these drugs are given in combination with a catechol-O-methyltransferase, or COMT inhibitor, called entacapone, that prevents the breakdown of levodopa by the enzyme COMT.
Very similarly, clients can be given MAO-B inhibitors like selegiline, which prevents the breakdown of dopamine by the enzyme monoamine oxidase B.
Finally, the dopamine agonist amantadine acts by increasing dopamine production. If medications fail to control symptoms or the client develops serious adverse effects, they can be treated with deep-brain stimulation.
This involves an implantable device that sends electrical signals to the brain that counteract the motor symptoms of PD. Okay, let’s get back and assess your client Michael.
After reviewing his chart, you enter his room, introduce yourself to Michael and his daughter, wash your hands, and confirm his identity. Michael is sitting in an armchair in a forward leaning posture.
You ask Michael how he is feeling today, and he replies “OK.” You note that he has a flat affect and is slow to respond to questions. A tremor in his right hand is also present.