Physical assessment - Ears: Nursing
Physical assessment - Ears: Nursing
421
421
Notes
| PHYSICAL ASSESSMENT - EARS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| GETTING STARTED |
| |
| ANATOMICAL LANDMARKS |
| |
| METHODS OF ASSESSMENT |
| |
| INSPECTION |
| |
| PALPATION |
| |
| SPECIAL TESTS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
Assessment of the ears should be completed as part of a comprehensive client assessment, or as part of a focused exam if the client is experiencing issues such as ear pain or hearing loss. This assessment gives the nurse information about hearing and equilibrium while helping to identify ear problems, such as otitis media. Let’s review the process of completing an ear assessment.
Okay, the supplies you’ll need for the ear assessment include an otoscope, a penlight, gloves, and a good source of light. Then, prepare for the exam by ensuring your client is in a comfortable position, that your hands are warm, and that the temperature in the room is comfortable. Also remember to provide privacy by closing the door and curtains.
Before getting started, explain the procedure to your client and be sure to answer any questions they might have before obtaining verbal consent. Then, perform hand hygiene and collect your supplies.
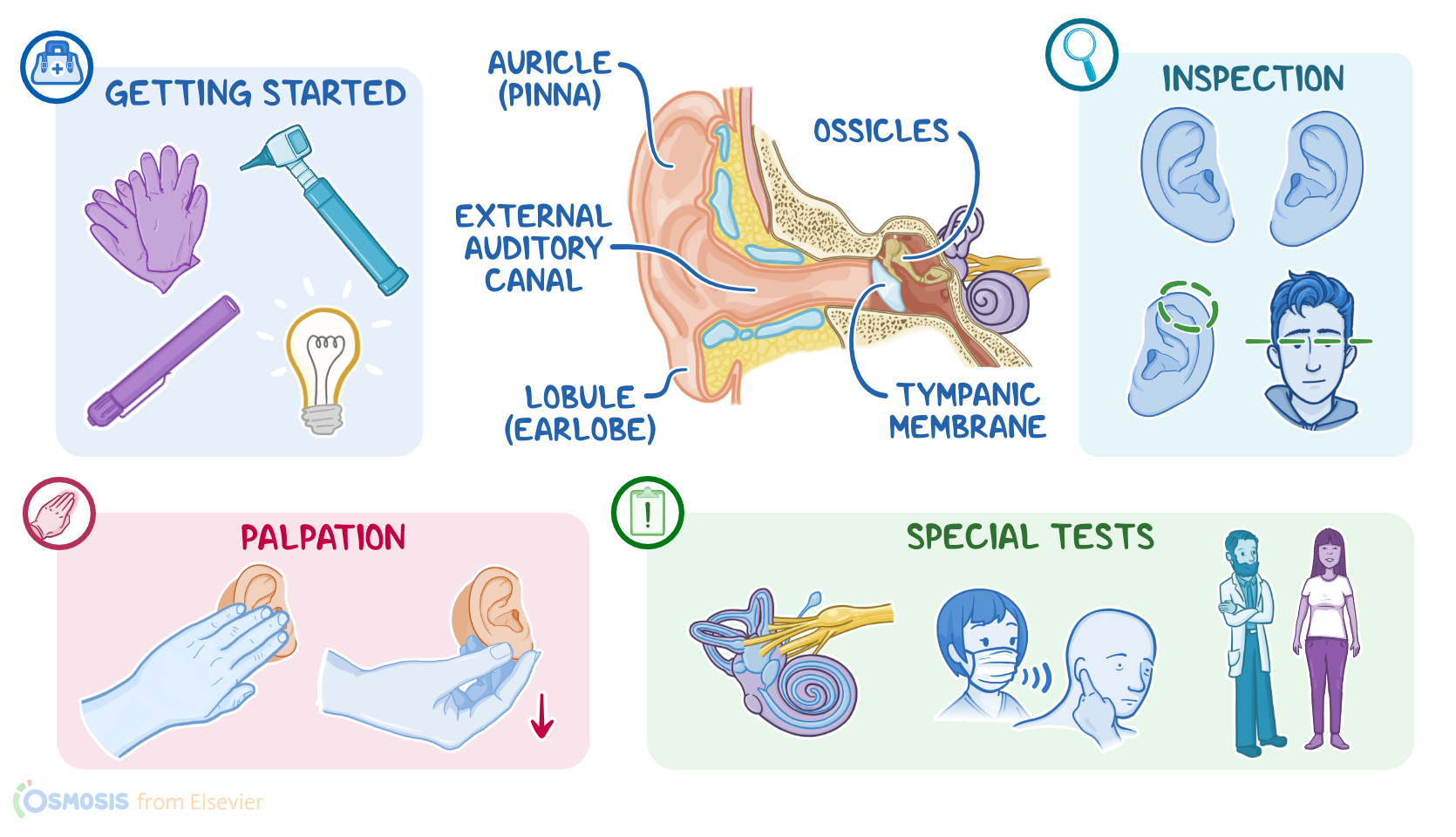
Now, locating the anatomical landmarks of the ears and surrounding tissue will help guide your assessment. The ear is divided into three sections: the external ear, middle ear, and the inner ear. Starting with the external ear, the landmarks include the auricle, also known as the pinna; the tragus; the lobule, or earlobe; the external auditory canal; and the mastoid process, which is the area directly behind the ear. Next, the middle ear contains the ossicles and the tympanic membrane which work together to transmit sound to the inner ear.
Alright, the methods of ear assessment include inspection and palpation as well as special tests, including the whisper test and the Romberg test.
First, you should inspect the external ear by viewing the auricles bilaterally, looking for size, shape, and symmetry. Also check that the skin on the auricles are the same color as their face. Be sure to inspect the position of the ears. Normally, the top of the auricle should align with the inner canthus of the eye. Clients with low-set ears may have a congenital abnormality. The ears should be free of lesions or nodules; however, a thickening of the upper helix of the auricle, called a Darwin tubercle, is an expected finding in some clients. Other ear abnormalities include cauliflower ear, tophi, or a sebaceous cyst. Cauliflower ear appears as an enlarged and thickened auricle and occurs from repeated trauma to the ear. Tophi are small white deposits of uric acid that appear along the auricles and are associated with gout. Sebaceous cysts indicate that the client has a blockage in their sebaceous glands, and appear as elevations in the skin around the ear.
Now, let’s move on to the external auditory canal, which should be free from drainage, odor, or excessive cerumen. You may need a penlight to view the canal, especially if your client has a buildup of cerumen. A foul smell or purulent drainage can be signs of otitis externa or may indicate the presence of a foreign body; whereas bloody drainage can be associated with trauma.