Physical assessment - Mental status: Nursing
Notes
| PHYSICAL ASSESSMENT - MENTAL STATUS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| GETTING STARTED |
| |
| METHODS OF ASSESSMENT |
| |
| APPEARANCE AND MOVEMENT |
| |
| BEHAVIOR |
| |
| COGNITION |
| |
| THOUGHT PROCESS |
| |
| SPECIAL TESTS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
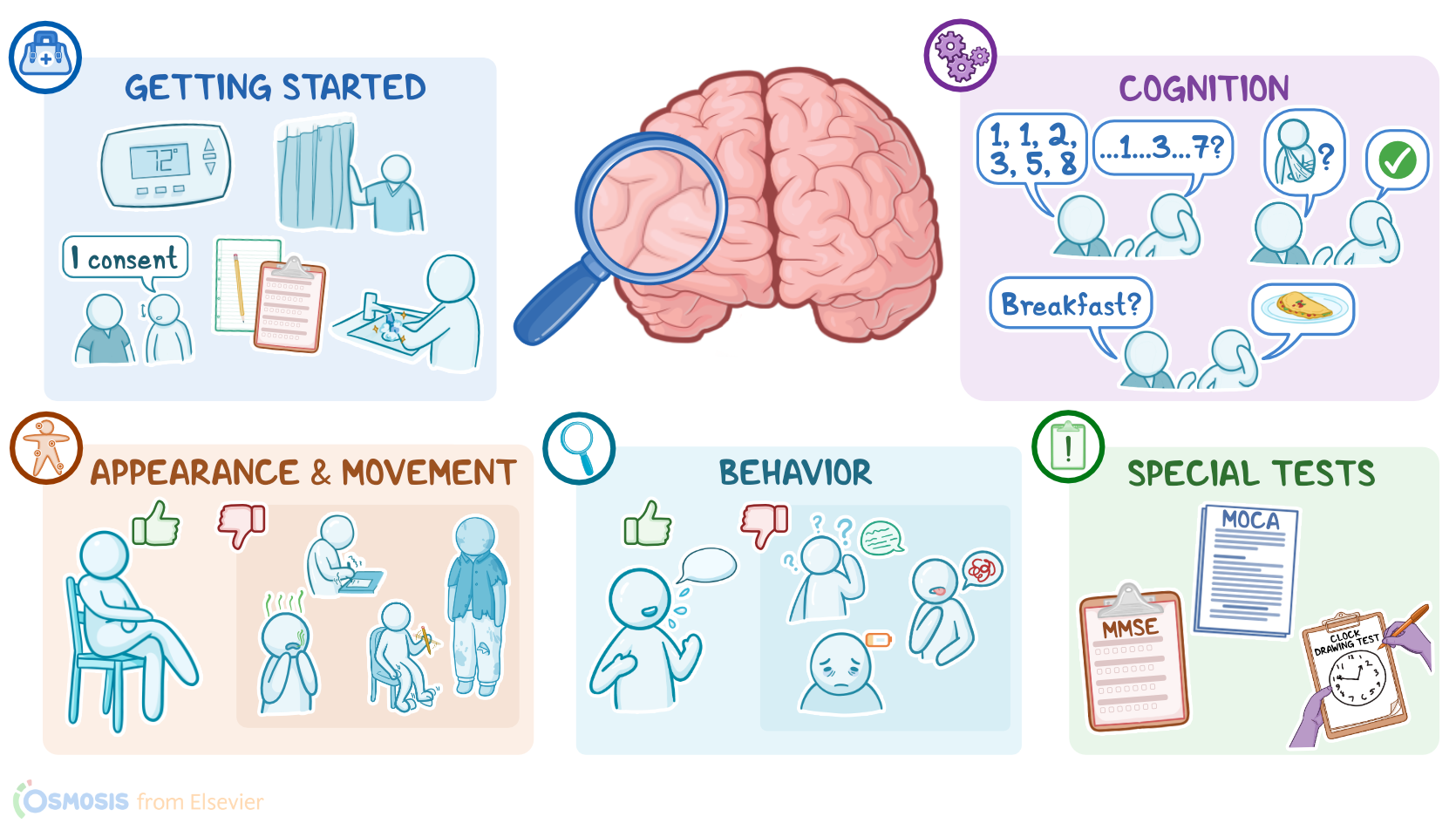
Mental status should be completed as part of a comprehensive assessment, or as part of a focused exam if a client is experiencing issues like confusion or memory loss. The mental status assessment provides the nurse with information about cognitive and emotional functioning. Let’s review the process of completing a mental status assessment.
Okay, so generally, you’ll need paper, pencil, and a copy of the mental status test you plan to administer. Then, prepare for the exam by ensuring your client is in a comfortable position, and that the temperature in the room is comfortable. Provide privacy by closing the door and curtains.
Before getting started, explain the procedure to your client and be sure to answer any questions they might have before obtaining verbal consent. Then, perform hand hygiene and collect your supplies. The method of assessment for a mental status exam is inspection.
First, let’s begin with appearance, which can be observed when your client moves into the exam room. When evaluating appearance, expect their posture to be erect and relaxed; and their movement should be smooth and purposeful. If your client appears restless or fidgety, this could be a sign of anxiety. Other unexpected findings include tics, which are sudden, repetitive movements like eye blinking or throat clearing; and tremors, which are rhythmic shaking movements.
Then, observe your client’s grooming. Expected findings include good hygiene, appropriate dress for the client’s age, season, and weather; and there should be no obvious hygiene issues such as body or breath odor. Inappropriate dress or evidence of poor hygiene might indicate conditions like depression or cognitive disturbances like dementia.
Next, assess your client’s behavior, beginning with their level of consciousness. Your client should be awake, alert, oriented, and responsive to both internal to environmental stimuli. Unexpected findings include lethargy or drowsiness; or being obtunded, meaning your client has a diminished response to environmental stimuli. Also observe your client’s facial expressions, which can tell you a lot about their emotional state. Their expressions should vary throughout the conversation and be appropriate to the context. A client who does not show much emotion through facial expressions exhibits a flat affect, which is a characteristic sometimes seen in clients with Parkinson disease or schizophrenia. On the other hand, your client is labile if they exhibit a rapid shift in facial expressions and emotions, a common finding in bipolar disorder.
Then, assess your client’s speech, paying attention to their tone, pace, word choice, and articulation. Their speech should be effortless with appropriate variations in tone. If your client has difficulty articulating words, this is known as dysarthria, and can be caused by conditions related to dysfunction of the central nervous system. Other unexpected findings include dysphonia, or an abnormal pitch or volume, which can be related to laryngeal disease; and aphasia, meaning there’s a problem with either the production or understanding of language.