Pleural effusion: Nursing
1,527views
Pleural effusion: Nursing
Acute Final
Acute Final
Notes
| PLEURAL EFFUSION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
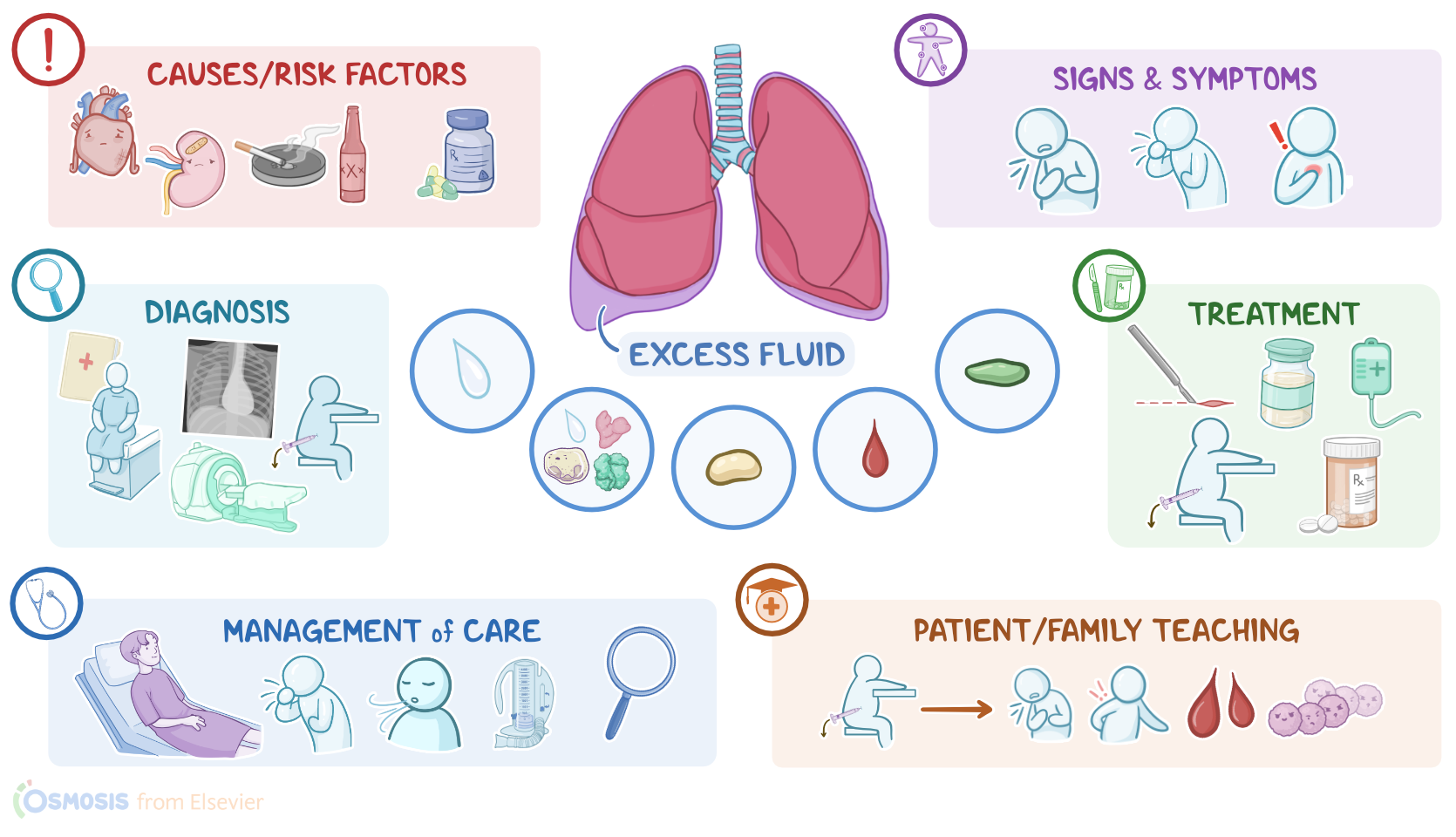
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Pleural effusion is a condition in which excess fluid accumulates in the space between the visceral layer and parietal layer of the pleura, called the pleural space.
Normally, this space contains 20 to 25 milliliters of fluid that provides lubrication, allowing the two pleural layers to slide over each other during breathing. This pleural fluid forms as a filtrate from pleural blood vessels. At the same time, it is drained into the lymphatic vessels, and this allows for regular renewal of the fluid.
Now, pleural effusion is typically caused by increased production or impaired drainage of the pleural fluid. Depending on the cause, the excess fluid in pleural effusion can be protein-poor, called transudate, or protein-rich, called exudate.
Transudate, also called hydrothorax when it involves the pleural space, forms when too much fluid starts to move from the pulmonary capillaries into the pleural space, either because of increased hydrostatic pressure or decreased oncotic pressure within the pulmonary capillaries. So increased hydrostatic pressure occurs usually in the context of heart failure, where the heart can’t pump blood effectively, so it backs up into the pulmonary vessels, leading to pulmonary hypertension; ultimately, the high pressure forces fluid out of the pulmonary capillaries and into the pleural space. On the other hand, decreased oncotic pressure can be caused by cirrhosis, which leads to decreased hepatic production of plasma proteins like albumin; or nephrotic syndrome, where renal filtration of blood is impaired, so the proteins are lost in urine.
On the other hand, exudate forms when there’s increased permeability of the pulmonary capillaries, which allows fluid, immune cells, and large proteins, along with lactate dehydrogenase or LDH, to leak out of the capillaries and into the pleural space. This can be caused by trauma, malignancy, such as lung cancer, inflammatory conditions like pancreatitis, and systemic lupus erythematosus, or an infection like pneumonia.
Additionally, in some cases, the fluid could be purulent, meaning it contains pus, which is called an empyema or pyothorax, and is usually caused by bacterial infection like pneumonia; or the fluid could be sanguineous, meaning it contains blood, called a hemothorax, and it’s usually caused by blunt chest trauma, as well as malignancy, or pulmonary embolism; or it could contain lymph, which is called a chylothorax, and it can be caused by lymphatic system injury from trauma or medical procedures. So, risk factors for pleural effusion include underlying heart, lung, kidney, or liver conditions, as well as exposure to tobacco smoke, alcohol, and the use of certain medications, such as immunosuppressants.
Now, the excess fluid building up in the pleural space puts pressure on the lungs and its surrounding structures, like the trachea for example, which may cause impaired ventilation or oxygenation. In addition, impaired drainage of pleural fluid causes this fluid to stagnate, which allows bacteria to grow and cause infections.
Now, a small pleural effusion typically causes no clinical manifestations. With larger pleural effusions, though, clients may present with dyspnea, dry cough, and sharp pain that comes with inspiration. During auscultation, there are reduced or absent breath sounds on the affected side. On percussion, there is dullness due to the presence of fluid within the pleural space.
The diagnosis of pleural effusion starts with the client’s history and physical assessment, followed by a chest X-ray or CT scan to visualize the effusion. A large effusion might also show a collapsed lung.
Diagnostic thoracentesis is frequently also done, which is a procedure that involves the collection of fluid from the pleural space to determine its composition and find out its cause. The main difference is that exudative effusions are rich in protein or LDH, while transudative effusions aren’t. So to definitively determine if the fluid is exudative or transudative, the Light’s criteria can be used.
Pleural fluid is considered exudative if any one of following are met: a pleural fluid total protein to serum total protein ratio more than 0.5, a pleural fluid lactate dehydrogenase, or LDH, to serum LDH ratio more than 0.6, or a pleural fluid LDH more than two-thirds of the upper limit of normal serum LDH. It’s very important to not miss an exudative effusion, so the criteria are designed to be overly sensitive. Now if none of the Light’s criteria apply, it’s a transudative effusion. In that case, it’s okay to treat the underlying cause, and no further tests are needed.