Pulmonary contusion: Nursing
Notes
| PULMONARY CONTUSION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
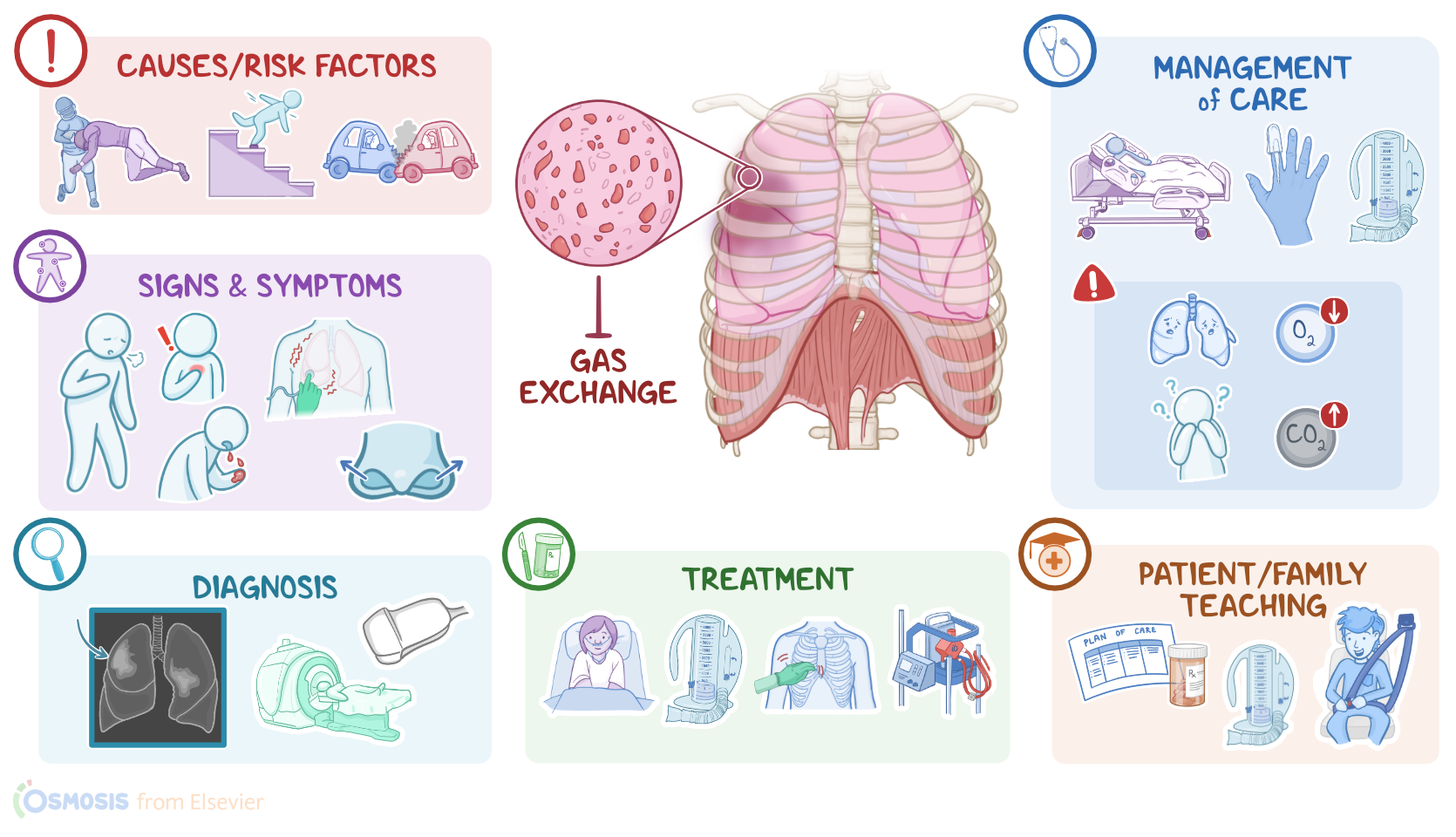
Pulmonary contusion is a lung injury that develops after chest trauma, and is characterized by interstitial hemorrhage that inhibits gas exchange.
Now, let’s quickly review the lower respiratory tract, which includes the lower part of the trachea, and the lungs containing the bronchi, bronchioles, alveolar ducts, and finally the alveoli. Alveoli are tiny air-filled sacs that are surrounded by tiny blood vessels, called capillaries.
If we zoom in even more, we can see a tiny space between the alveolar wall and the capillary wall, called the interstitial space, which normally contains a small amount of interstitial fluid. And that’s where most gas exchange occurs, so as we breathe, the inhaled oxygen moves through the alveolar membrane, the interstitial space, and the capillary membrane to reach the blood, while the carbon dioxide moves from the capillaries through the interstitial space and into the alveolar sacs to be exhaled.
Now, the alveoli are lined by alveolar epithelial cells, called pneumocytes. The vast majority are type I pneumocytes, which allow oxygen and carbon dioxide to pass through them. There are also type II pneumocytes scattered around which produce surfactant, an oily secretion that coats the alveoli and prevents their collapse.
The main cause of pulmonary contusion is direct blunt trauma to the chest. Risk factors for pulmonary contusion typically include car crashes, falls from heights, child abuse, and sport injuries. Clients who serve in the military are also at an increased risk of pulmonary contusions, due to blast injuries from explosives.
Okay, let’s look at what happens when the force from the chest injury reaches the lung parenchyma. Well, first, there’s tearing of the alveolar and capillary membrane, which causes blood and interstitial fluid to leak into the alveolar space, preventing gas exchange. At the same time, immune cells start producing pro-inflammatory cytokines which trigger inflammation and edema of the interstitial space, inhibiting gas exchange even more.
Meanwhile, damaged type II pneumocytes stop producing surfactant, causing alveolar collapse. These collapsed, fluid-filled alveoli cannot participate in gas exchange, causing reduced lung volume, and shunting, where blood doesn't become oxygenated as it moves through the lungs. This can ultimately result in acute respiratory distress syndrome, or ARDS, which is a life-threatening complication characterized by extreme hypoxemia and respiratory failure. Other complications include pneumothorax and hemothorax, where air or blood leak into the pleural space surrounding the lungs, respectively.
Now the clinical manifestations of pulmonary contusion vary based on the extent of lung injury. Initially, clients might be asymptomatic. Over time, as the disease progresses, a client may experience shortness of breath, cough, hemoptysis, chest pain, and respiratory distress, which presents as short, shallow, and rapid breathing, along with nasal flaring and retractions.
During auscultation, there are diminished breath sounds on the affected side. Crackles can also sometimes be heard, which is the sound of collapsed alveoli popping open with inspiration. On percussion, there’s dullness over the affected area, and on palpation, there is often localized tenderness and sometimes decreased fremitus. Arterial blood gas, or ABG analysis may show hypercarbia and respiratory acidosis.
Diagnosis of pulmonary contusion involves the client’s history and physical assessment, followed by a chest X-ray, which shows areas of ground-glass haziness of the lung, which is usually not visible until at least 6 hours after the injury. Additional imaging studies, such as an ultrasound, or a CT scan, might also be helpful.
Treatment of pulmonary contusion focuses on supportive care for breathing. For mild injuries, clients can be treated with supplemental oxygen, encouraging coughing and deep breathing exercises, using an incentive spirometer, or with chest physiotherapy which includes chest percussion and postural drainage to help clear the airways;
If needed, positive pressure ventilation with continuous positive airway pressure or CPAP; bi-level positive airway pressure or BiPAP; or mechanical ventilation with positive end-expiratory pressure or PEEP, can be used, which is where the pressure in the lungs is kept slightly above atmospheric pressure, even after exhalation, because that helps prevent the alveoli from collapsing.