Rheumatoid arthritis (RA): Nursing process (ADPIE)
Rheumatoid arthritis (RA): Nursing process (ADPIE)
Watch later
Watch later
Notes
| RHEUMATOID ARTHRITIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Clara Reed is a 44-year-old female client who presents to the rheumatology clinic after being referred by her primary care physician. For the past several weeks, she has been having pain, stiffness and swelling in both hands along with stiffness in her body that is worse in the morning. She has also been feeling fatigued and her appetite has decreased.
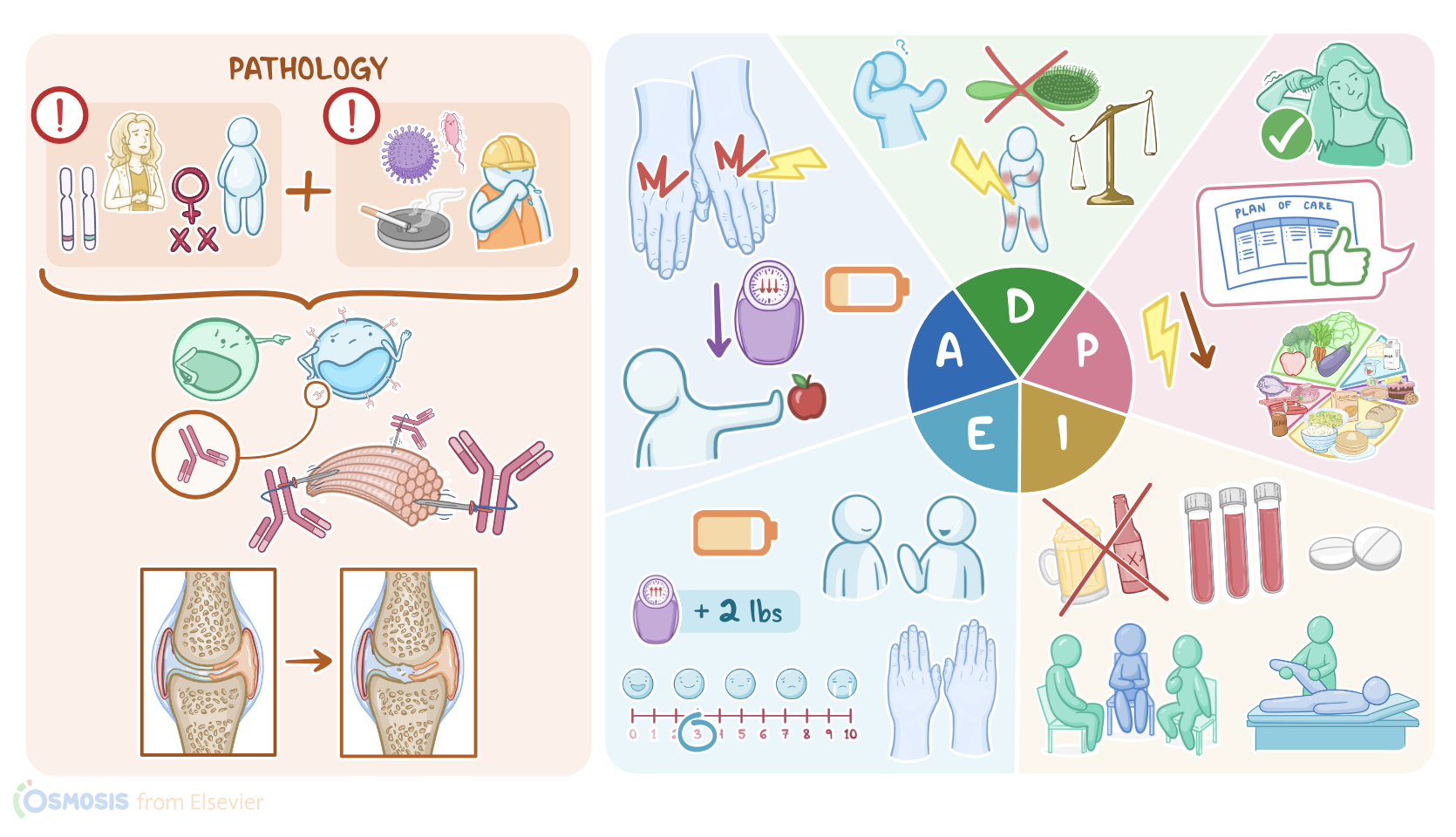
Alright, so rheumatoid arthritis is a chronic, autoimmune, inflammatory disorder that mostly affects the joints, but can also involve other organ systems like the skin and lungs. This condition is typically triggered by an interaction between genetic and environmental factors. Rheumatoid arthritis tends to run in families and it’s been associated with the HLA-DR4 gene. Other risk factors include being female, middle aged, and obese. Finally environmental factors like infections, smoking, and exposure to asbestos and silica are also linked to the disease.
A person with the HLA–DR4 gene, might develop rheumatoid arthritis after getting exposed to something in the environment like cigarette smoke or a specific pathogen. These environmental factors can cause modification of the proteins in our body and turn them into antigens that trigger the immune system to produce specific autoantibodies against them.
The first antibody is called rheumatoid factor, or RF, and targets modified IgG antibodies; whereas the second antibody is called anti-cyclic citrullinated peptide antibody or anti-CCP, and targets citrullinated proteins, like citrullinated collagen II.
Next, these antibodies and immune cells enter the circulation and reach joints. Here, immune cells release inflammatory cytokines that induce inflammation and stimulate synovial cells to proliferate. Increased number of synovial and immune cells in the joint creates a pannus, which is a thick synovial membrane with granulation tissue.
Over time, the cytokines released in the pannus start to damage the articular cartilage, leaving the underlying bone exposed. As a result, bones start to directly rub against one another, eventually causing bone erosion. Meanwhile, the antibodies that enter the joint space bind to their targets and form immune complexes that accumulate in the synovial fluid, activating the complement system and inducing further destruction of the joint.
Now, rheumatoid arthritis is a symmetric and progressive condition, associated with articular and extra-articular manifestations. Articular manifestations include pain, swelling, and loss of mobility in the affected joints. Also, there's no redness or warmth because the inflammatory process is gradual, but there’s morning stiffness that typically improves after 30 minutes of movement.
Most commonly, rheumatoid arthritis affects the proximal interphalangeal and metacarpophalangeal joints of the hand. Distal interphalangeal joints are rarely involved because they have very little synovium. In the feet, the metatarsophalangeal joints are usually affected, which causes a person to bear more weight on the heels and hyperextend the toes.
Other joints that can be involved are the shoulders, elbows, wrists, knees, and ankles. Hip involvement can occur later in the disease, and it’s characterized by pain in the groin, thigh, or lower back. Finally, if rheumatoid arthritis affects the C1-C2 joint, which is the only synovial joint in the spine, it can cause quadriplegia, which is the loss of use of all extremities.
On the flip side, extra-articular symptoms include fever, fatigue, weakness, and a loss of appetite that can eventually lead to weight loss.
Rheumatoid arthritis can also lead to vasculitis and the formation of atheromatous plaques, which can break off and cause myocardial infarction or stroke. In fact, cardiovascular disease is the main cause of mortality in individuals with rheumatoid arthritis.
In skeletal muscle, inflammation can lead to muscle breakdown, and in the skin, inflammation can cause the formation of rheumatoid nodules over bony prominences.
Rheumatoid arthritis is also associated with carpal tunnel syndrome, which refers to the compression of the median nerve on its way through the wrist, through a narrow passageway called the carpal tunnel.
In the lungs, clients might develop pulmonary fibrosis or scarring of the lung tissue, and pleural effusion, which is an accumulation of fluid in the pleural space. Finally, the destruction of bones and skeletal system increases the risk of osteoporosis.
Diagnosis is based on clinical examination and blood tests, which typically reveal low red blood cell count, in combination with elevated erythrocyte sedimentation rate, or ESR and C-reactive protein, often referred to as CRP. Moreover, these findings are commonly seen in conditions associated with chronic inflammation. Additionally, these clients should be tested for rheumatoid factor and anti-cyclic citrullinated peptide antibodies.
Sources
- "Global, regional, and national burden of rheumatoid arthritis, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021" Lancet Rheumatol (2023)
- "Update on the Pathomechanism, Diagnosis, and Treatment Options for Rheumatoid Arthritis" Cells (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Robbins & Kumar Basic Pathology, 11th edition" Elsevier (2022)
- "Pathogenesis of rheumatoid arthritis: one year in review 2022" Clin Exp Rheumatol (2022)
- "Management of Rheumatoid Arthritis: An Overview" Cells (2021)
- "The etiology of rheumatoid arthritis" J Autoimmun (2020)