Suicide: Nursing
Suicide: Nursing
Psych Final
Psych Final
Notes
| SUICIDE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
The word suicide comes from the Latin word suicidim, which literally means the act of ending one’s own life. A suicidal attempt is an attempt to end one’s own life that results in survival; while suicidal ideations are thoughts about suicide.
First, let’s cover some basic physiology of the brain, which contains several types of neurons, including serotonergic neurons, which release serotonin; dopaminergic neurons, which release dopamine; and noradrenergic neurons, which release norepinephrine. Overall, all these neurotransmitters, as well as several others and various factors like home and social environment, to name a few, play a key role in the delicate balance of mental functions, and influence things like memory, behavior and mood, amongst others.
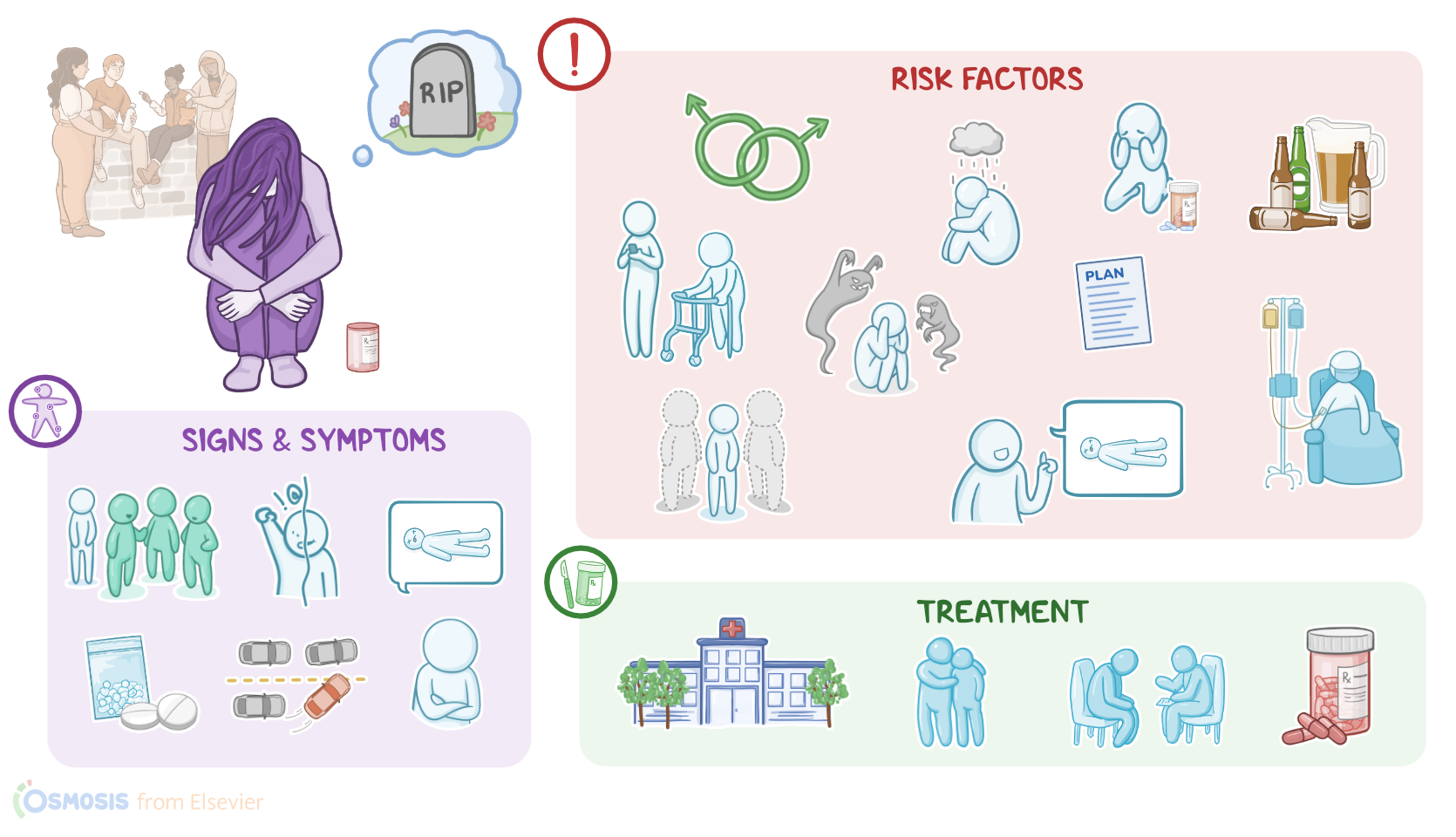
Now, let’s switch gears and move on to risk factors, which can be easily remembered with the memory trick: SAD PERSONS. The first S here stands for sex, as suicide tends to be more common among those assigned male at birth. Next, A stands for age, since suicide is more common among young adults and the elderly. D is for depressive disorder, which is a mental health condition that causes a persistent feeling of sadness, associated with a loss of interest in everyday activities like hobbies. Then P stands for previous suicide attempts, which is the most important risk factor for suicide. E stands for excessive use of alcohol or substances, which causes clients to be more impulsive, and take risks they normally wouldn’t take, like driving recklessly. R is for rational thinking loss in psychosis, a severe mental health disorder that can impair thought and emotions, to the point where clients lose touch with reality. The next S is for sickness, which refers to chronic non-psychiatric diseases, like end-stage cance r. O stands for organized plan, which is when the client has a specific method for suicide in mind. Next, N stands for no social support, meaning that they have no friends or family to turn to during vulnerable times. The last S refers to stated future intent, which is when a client expresses their suicidal thoughts or intentions.
On the other hand, protective factors, which can decrease the risk of suicide,can be either internal or external. Internal factors include the client’s tolerance to frustration and stressful situations; use of good coping skills, like meditation; a sense of purpose; and religious and cultural beliefs that discourage suicide. On the flip side, external protective factors include access to health care; social and emotional support, like having family, friends, or partner; responsibility to another family member or even a pet; and finally, restricted access to weapons or other lethal means.
The exact pathology of suicidal behavior remains unknown. Some sources suggest that it might be associated with neurotransmitter imbalance and disrupted dopaminergic, noradrenergic, and serotonergic systems, which are commonly affected in mental health conditions, such as depression. Additionally, clients who present with impulsive and suicidal behavior typically have low cerebrospinal fluid levels of the serotonin metabolite called 5-hydroxyindoleacetic acid. Finally, some evidence suggests a possible connection between the overactivity of the hypothalamic-pituitary-adrenal axis and an impaired stress response mechanism and suicidal behavior.
Clinical manifestations of suicidal behavior vary from client to client, but the most important ones include social isolation, frequent mood swings, and conversations about dying, death, and suicide. For example, some clients can directly express suicidal thoughts and say things like “I’m going to end my life” or “I wish I was dead". Other important signs include changes in eating or sleeping routines, and high-risk behavior, like using substances, reckless driving, and excessive alcohol drinking. Finally, it’s important to note that some clients can present with no observable signs of suicidal behavior.
Diagnosis is based on the client’s history and screening tools, such as Suicide Assessment Five-step Evaluation or SAFE-T for short. This five-step evaluation plan is used to identify risk factors; identify protective factors; identify thoughts, plans, and intent for suicide, and, finally, determine levels of risk and intervention. The last step includes documentation of the treatment plan. Other commonly used screening tools include Columbia-Suicide Severity Rating Scale, or C-SSRS for short; and Patient Health Questionnaire 9, or PHQ-9 for short. Finally, the management of suicidal behavior can be either short-term or long-term. Short-term management includes hospitalization for clients with an imminent risk of suicidal behavior; and increased social support for clients with a possible risk of suicidal behavior.
On the other hand, long-term management can be either non-pharmacological and pharmacological. Non-pharmacological management includes crisis intervention, counseling, and reduction of current risk factors, improvement of the current life situation, and development of coping skills. On the flip side, pharmacological management can be used for clients with an underlying mental health condition and includes the use of medications such as mood stabilizers, antidepressants, and antipsychotics.