Mobitz type II is a type of 2nd degree AV block, which refers to an irregular cardiac rhythm (i.e., arrhythmia) caused by a block in the electrical conduction system of the heart.
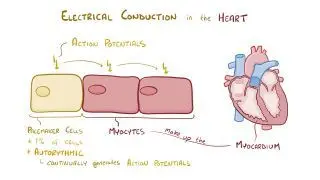
The heart is a muscular organ composed of four chambers: two upper chambers (the right and left atria) and two lower chambers (the right and left ventricles). The chambers of the heart are wired with an electrical conduction system much like the electrical system of a house. This system consists of the sinoatrial (SA) node, the atrioventricular (AV) node, the bundle of His, the right and left bundle branches, and the Purkinje fibers. These conduction pathways are a network of highly specialized cells that generate and conduct electrical impulses, allowing the heart to contract rhythmically and pump out blood with each heartbeat.
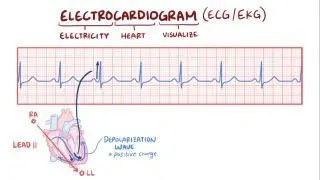
The heart’s electrical activity can be monitored with an electrocardiogram (ECG), which uses several electrodes (i.e., leads) placed on the patient’s limbs and chest to register the heart’s electrical activity from different angles. Electrical signals are first fired at the SA node where they then travel through the walls of the atria, triggering atrial contraction and the consequent movement of blood into the ventricles. During atrial contraction, the ECG will show a small deflection from the basal line called the P wave. Next, the electrical signal is conducted through the AV node and then to the ventricles through the bundle of His and Purkinje fibers. This triggers ventricular contraction, which pushes blood out of the heart and into circulation, resulting in a larger set of waves on the ECG that form the QRS complex. The interval between the onset of the P wave and QRS complex is known as the PR interval and reflects the typical slowed conduction through the AV node. After the QRS complex, there’s another deflection called the T wave, which corresponds to the relaxation and repolarization of the ventricles.
An
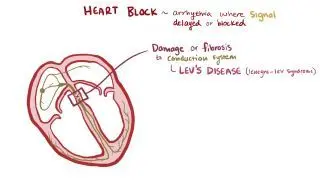
atrioventricular block (AV block), also known as a
heart block, occurs when an atrial impulse gets delayed or completely blocked at some point along the electrical conduction system of the heart. There are three degrees of AV block, according to the location and severity of the nodal block. A 1
st degree AV block is not technically a block but rather a delay in the conduction of atrial impulses to the ventricles, which results in a prolonged PR interval. Meanwhile, a 2
nd degree AV block, which can be further divided into Mobitz I and Mobitz II, occurs when some of the atrial impulses are fully conducted to the ventricles, whereas others are blocked along the way. Blocked atrial impulses can be seen on an ECG as a P wave that is not followed by a corresponding QRS complex, resulting in a slowed
heart rhythm (i.e.,
bradycardia) and/or missed
heart beats. Finally, a 3
rd degree AV block occurs when none of the atrial impulses are conducted, leaving the atria and ventricles completely disconnected from one another. On the ECG, it can be detected by a total lack of
correlation between the P waves and
QRS complexes.