Mobitz Type I · What Is It, Causes, Signs and Symptoms, Diagnosis, Treatment, and More
Published: Mar 04, 2025
Author: Anna Hernández, MD•
Editor: Ahaana Singh•
Editor: Lisa Miklush, PhD, RN, CNS
Illustrator: Aileen Lin
7-day free trial
Go deeper with Osmosis
Osmosis is a learning platform with videos, questions, and AI tools to help you master topics like this.
Watch quick, visual videos
Practice with Qbank-style questions
Use AI to explain, quiz, and review
Study anytime with the mobile app
No credit card · Cancel anytime
What is Mobitz type I?
Mobitz type I is a type of 2nd degree AV block, which refers to an irregular cardiac rhythm (arrhythmia), that reflects a conduction block in the electrical conduction system of the heart.
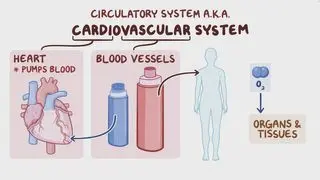
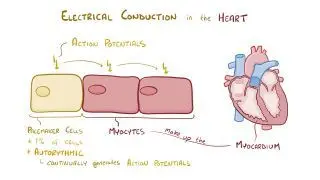
The heart is a muscular organ composed of four chambers: two upper chambers—the right and left atria—, and two lower chambers— the right and left ventricles. The chambers of the heart are wired with an electrical conduction system much like the electrical system of a house. This system consists of the sinus node, the atrioventricular (AV) node, the bundle of His, the right and left bundle branches, and Purkinje fibers. These conduction pathways are a network of highly specialized cells that generate and conduct electrical impulses, allowing the heart to contract rhythmically and pump out blood with each heartbeat.
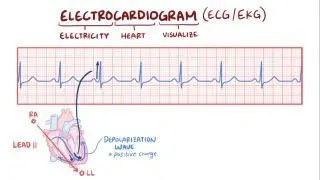
The heart’s electrical activity can be monitored with an electrocardiogram (ECG), which uses several electrodes (leads) to register the heart’s electrical activity from different angles. Electrical signals are first fired at the sinus node, where they then travel through the walls of the atria, triggering atrial contraction and the consequent movement of blood into the ventricles. During atrial contraction, the ECG will show a small deflection of the basal line, called the “P wave”. Next, the electrical signal is conducted through the AV node and then to the ventricles through the bundle of His and Purkinje fibers. This triggers ventricular contraction which pushes blood out of the heart and into circulation, resulting in a larger set of waves on the ECG that form the “QRS complex”. The interval between the onset of the P wave and QRS complex is known as the “PR interval”, and reflects the typical slowed conduction through the AV node. After the QRS complex, there’s another deflection called the “T wave”, which corresponds to the relaxation of the ventricles.
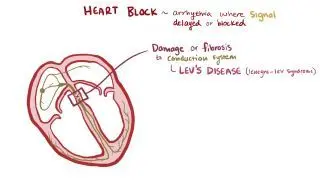
An atrioventricular block (AV block), also known as a heart block, occurs when an atrial impulse gets delayed or completely blocked at some point along the electrical conduction system of the heart. There are three degrees of AV block, according to the location and severity of the nodal block. A 1st degree AV block is not technically a block, but rather a delay in the conduction of atrial impulses to the ventricles, which results in an extended PR interval. Meanwhile, a 2nd degree AV block occurs when some of the atrial impulses are fully conducted to the ventricles, whereas others are blocked along the way. Blocked atrial impulses can be seen as a P wave that is not followed by a QRS complex, resulting in an irregular cardiac rhythm. Finally, a 3rd degree AV block occurs when none of the atrial impulses are conducted, leaving the atria and ventricles completely disconnected from one another. On the ECG, it can be detected by a total lack of correlation between the P waves and QRS complexes.Learn deeper with Osmosis
Master this topic faster with videos, questions, and AI.
Used by 8M+ healthcare learners.
Start free trial
No credit card · Cancel anytime
Are Wenckebach and Mobitz type I the same thing?
Yes, Mobitz type I is also known as Wenckebach block or 2nd degree heart block type I. All three names refer to the same ECG rhythm and can be used interchangeably.
What is the difference between Mobitz I and Mobitz II?
Mobitz I and Mobitz II are both subtypes of a 2nd degree AV block. Mobitz I and Mobitz II can be distinguished on an ECG by the pattern in which P waves are blocked; in Mobitz I, there is a progressive prolongation of the PR interval until a P wave fails to conduct, whereas in Mobitz II, PR intervals are always the same length, but are followed by a pattern of one or more non-conducted P waves.
Mobitz I and Mobitz II also differ in the severity of the conduction block. Mobitz I is a benign rhythm that generally reflects a block at the AV node, and typically results in a good prognosis. On the other hand, Mobitz II reflects a block after the AV node, either at the bundle of His or its branches, and often results in a poorer prognosis, as it has a higher risk of progressing to a 3rd degree AV block.
Mobitz I and Mobitz II also differ in the severity of the conduction block. Mobitz I is a benign rhythm that generally reflects a block at the AV node, and typically results in a good prognosis. On the other hand, Mobitz II reflects a block after the AV node, either at the bundle of His or its branches, and often results in a poorer prognosis, as it has a higher risk of progressing to a 3rd degree AV block.
What are the causes of Mobitz type I?
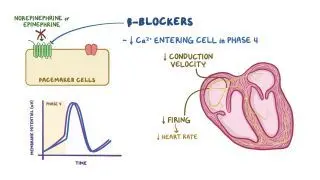
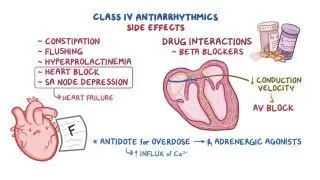
Mobitz type I block can occur as a result of a reversible conduction block caused by metabolic abnormalities, such as increased levels of potassium in the blood (hyperkalemia), medications that slow nodal conduction (e.g. digoxin, beta-adrenergic blockers, calcium-channel blockers, amiodarone), or increased parasympathetic activation of the nervous system (increased vagal tone), which is often seen in healthy athletes. Other causes of Mobitz type I block include a heart attack, disorders affecting the heart muscle walls (cardiomyopathies), inflammation of the heart muscle (myocarditis), infection of the inner layer of the heart (endocarditis), inherited heart defects, infiltrative and autoimmune disorders, and cardiac surgical procedures.
What are the signs and symptoms of Mobitz type I?
Most people with Mobitz type I block do not present any symptoms. Some individuals may occasionally feel light-headedness, dizziness, or fatigue when exercising. More rarely, Mobitz type I block may lead to a sudden and temporary loss of consciousness, also known as a syncope, caused by a brief decrease in the oxygen supply to the brain.
How is Mobitz type I diagnosed?
Mobitz type I block is often diagnosed incidentally during a routine ECG. The key to diagnosing Mobitz type I block is looking closely at the PR interval on the ECG strip. In Mobitz I, the sinus node is healthy and fires right on time, so the P waves come at regular intervals. However, atrial impulses travelling through the AV node take longer and longer to conduct at each subsequent impulse, causing a progressive prolongation of the PR interval, until one impulse is completely blocked. Consequently, QRS complexes are periodically dropped, which can result in a slowed heart rhythm (bradycardia), with more P waves than QRS complexes on the ECG.
How is Mobitz type I treated?
Treatment of Mobitz type I begins by addressing any potentially reversible causes of nodal block, including ceasing medications that can slow nodal conduction and correcting any electrolyte imbalances, such as with hyperkalemia. Electrolyte imbalances can be corrected by administering intravenous (IV) fluids or with the use of certain medications. If the AV block is a result of another heart condition, treatment may also include addressing the specific cause, when possible. Some symptomatic individuals may also benefit from treatment with medications that temporarily improve conduction through the AV node, such as atropine. Finally, individuals with persisting symptoms or those at high risk of developing an advanced heart block may benefit from placement of a temporary or permanent cardiac pacemaker.
What are the most important facts to know about Mobitz type I?
Mobitz type I, also known as Wenckebach block, is a type of 2nd degree AV block, which refers to a cardiac arrhythmia that reflects a conduction block at the atrioventricular AV node. In Mobitz type I, atrial impulses travelling through the AV node take increasingly longer to fully conduct to the ventricles, until one impulse is completely blocked. On the ECG, this can be seen as a progressive prolongation of the PR interval, until a P wave is not followed by a QRS complex. Individuals with Mobitz type I block are generally asymptomatic, although some individuals may feel fatigue, lightheadedness, or dizziness. Causes of Mobitz type I block include medications, electrolyte imbalances, increased vagal tone, and structural disorders of the heart. Treatment begins by addressing any potentially reversible causes and underlying heart conditions, when possible. In asymptomatic individuals, further treatment is usually not necessary. On the other hand, symptomatic individuals may benefit from medications that temporarily increase nodal conduction or, alternatively, placement of a temporary or permanent cardiac pacemaker.
Related topics
Students say Osmosis is 100% worth it
Because Osmosis saves them time. Lowers stress. And actually helps them remember when it counts.
I used Osmosis to prepare for my first medical school licensing exam! Super helpful and interactive for people who may not do great with just pages of text info!
Cecilia Ruiz
MD student

I have used Osmosis for about four years. Best thing I have ever used for my medical studies.
Sayan Misra
Med student
Osmosis videos are superior because they define simple concepts, tell a story with a clear progression, and provide context.
Jay Pate
Dental student