

Faraklas, I., Lam, U., Cochran, A., Stoddard, G., & Saffle, J. (2011). Colloid normalizes resuscitation ratio in pediatric burns. Journal of burn care & research, 32(1), 91–97. https://doi.org/10.1097/BCR.0b013e318204b379
Gomella, L. G., & Haist, S. A. (2007). Chapter 9. Fluids and electrolytes. In Clinician’s Pocket Reference: The Scut Monkey (11th ed.). The McGraw-Hill Companies. accessmedicine.mhmedical.com/content.aspx?aid=2701183
Mehta, M., & Tudor, G. J. (2022). Parkland formula. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK537190/
Romanowski, K. S., & Palmieri, T. L. (2017). Pediatric burn resuscitation: Past, present, and future. Burns & Trauma, 5, 26. https://doi.org/10.1186/s41038-017-0091-y
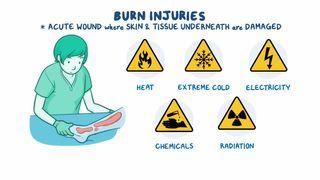
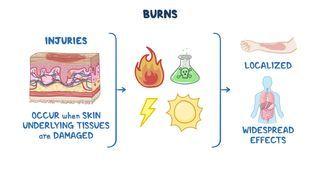
Warby, R., & Maani, C. V. (2022). Burn classification. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK539773/