
A child presents with recurrent infections. Which finding from a focused history or physical examination would be most helpful in supporting a diagnosis? Do you know the answer? Let’s find out!
A 5-year-old boy presents to clinic with a parent for evaluation of persistent eczema. Medical history is significant for frequent respiratory tract infections. Birth and family histories are non-contributory. Temperature is 37°C (98.6°F), pulse is 100/min, respirations are 22/min, blood pressure is 96/58 mm Hg, and oxygen saturation is 98% on room air. Physical examination reveals eczematous lesions over the elbows and knees with associated excoriation. No dysmorphic features are noted. Cardiopulmonary and abdominal examinations are normal. Laboratory studies are shown below.
| Laboratory value | Result |
| Serum chemistries | |
| Hemoglobin | 12 g/dL |
| Hematocrit | 40% |
| Leukocyte count | 9,100/mm3 |
| Platelet count | 80,000/mm3 |
A. Chediak-Higashi syndrome
B. DiGeorge syndrome
C. Hyper-IgE syndrome
D. Hyper-IgM syndrome
E. Wiskott-Aldrich syndrome
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
E. Wiskott-Aldrich syndrome
Correct: See Main Explanation.
Incorrect Answer Explanations
A. Chediak-Higashi syndrome
Incorrect: Chediak-Higashi syndrome may present with recurrent infections and bleeding due to platelet dysfunction, but it is typically associated with partial oculocutaneous albinism.
B. DiGeorge syndrome
Incorrect: Although this patient has recurrent infections, the absence of seizures and congenital heart defects, along with the presence of eczema and thrombocytopenia, makes DiGeorge syndrome less likely.
C. Hyper-IgE syndrome
Incorrect: Ezema is a common feature of Hyper-IgE syndrome. However, the absence of coarse facial features and the presence of thrombocytopenia are more consistent with Wiskott-Aldrich syndrome.
D. Hyper-IgM syndrome
Incorrect: Hyper-IgM syndrome is associated with recurrent opportunistic infections and may present with osteopenia, fractures, diarrhea, or inflammatory bowel disease. Eczema and thrombocytopenia are not characteristic findings.
Main Explanation
This child presents with eczema and recurrent respiratory tract infections. The initial evaluation reveals normal facies, eczematous skin, and thrombocytopenia, findings consistent with Wiskott-Aldrich syndrome (WAS).
Primary immunodeficiencies often present with recurrent, severe, or opportunistic infections. Additional clues may include an abnormal newborn screen, a personal history of autoimmune disease, or a family history of immunodeficiency. Poor growth and suboptimal weight gain may also be seen on the growth chart. When evaluating such patients, the next step is to look for characteristic clinical features that suggest a specific syndrome.
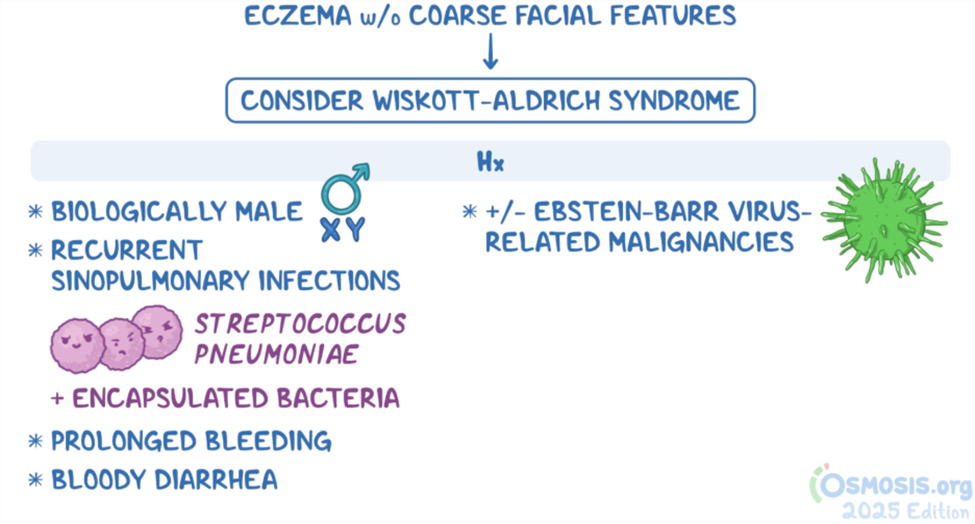
Eczema is seen in both Hyper-IgE syndrome and Wiskott-Aldrich syndrome (WAS). To help distinguish between them, assess for coarse facial features. If present, consider Hyper-IgE syndrome, which may also present with skin abscesses lacking overt inflammation. In contrast, eczema without coarse facies should raise concern for WAS.
WAS is an X-linked immunodeficiency characterized by recurrent sinopulmonary infections (particularly with Streptococcus pneumoniae), eczema, prolonged bleeding, bloody diarrhea, and abnormal lymphocyte function. Due to its X-linked recessive inheritance, most affected patients are biologically male. Clinical findings typically include eczema and purpura, and laboratory evaluation reveals thrombocytopenia, decreased IgM, elevated IgA and IgE, and sometimes decreased IgG. Diagnosis is confirmed with genetic analysis of the WASP gene.
Major Takeaway
Wiskott-Aldrich syndrome (WAS) is an X-linked recessive immunodeficiency typically affecting biologically male patients. It is characterized by recurrent sinopulmonary infections, eczema, prolonged bleeding due to thrombocytopenia, and abnormal lymphocyte function. Unlike Hyper-IgE syndrome, patients with WAS do not have coarse facial features.
Want to learn more about this topic?
Watch the Osmosis video: Approach to primary immunodeficiencies: Clinical sciences
References
- Kliegman, RM, St Geme, JW, Blum, NJ, et al, eds. Nelson Textbook of Pediatrics. 21st ed. Elsevier; 2020.
- Dosanjh A. Autoimmunity and Immunodeficiency. Pediatr Rev. 2015;36(11):489-495. doi:10.1542/pir.36-11-489

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply