Assessment - Postpartum: Nursing
Notes
| ASSESSMENT - POSTPARTUM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| COMPLICATIONS |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
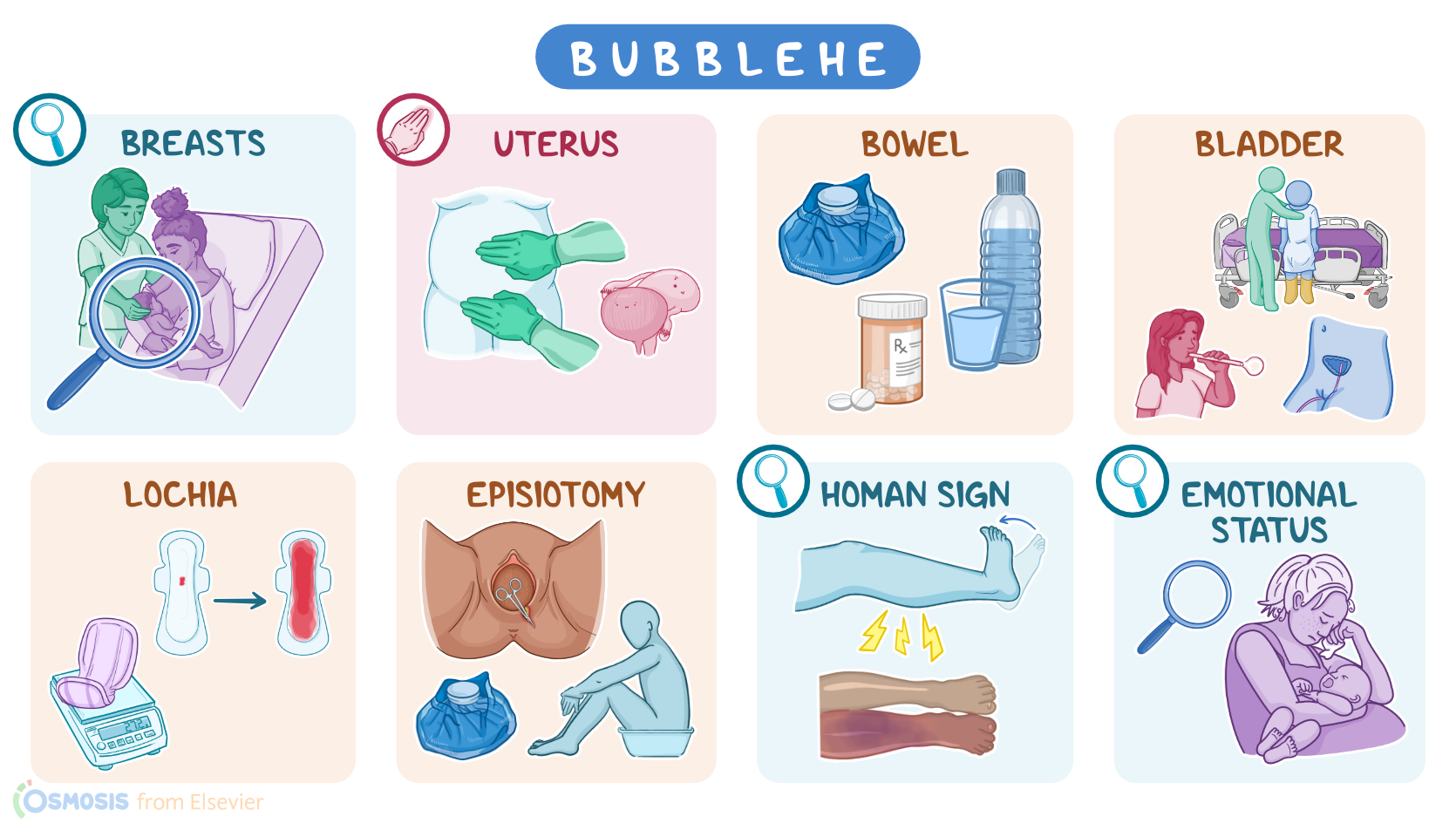
| NURSING ASSESSMENT |
| |
Transcript
The postpartum period, also known as the puerperium, or “the fourth stage of labor”, starts after delivery of the fetus and the placenta, and it extends through the first six weeks after birth. During this period, the body gradually returns to its pre-pregnancy state. There are several complications that can arise during the postpartum period, and early diagnosis is essential for appropriate management of these conditions.
Okay, let’s start with some physiology. So, after delivery, the uterus tends to regress back to its normal size and resume its pre-pregnancy position by the sixth week, a process known as involution. There are also some physiological changes that occur during pregnancy that begin to change back to pre-pregnancy levels in the postpartum period. For example, during pregnancy there is increased blood plasma volume in relation to red blood cell mass. As a consequence, maternal hemoglobin and hematocrit are usually relatively low during pregnancy, since the same amount of red blood cells are circulating in a higher volume of blood. After delivery, through increased diuresis or urine production, and increased diaphoresis or sweat production, blood volume returns to normal in about 6 to 12 weeks, and hemoglobin, and hematocrit levels normalize within 4 to 6 weeks. Likewise, during pregnancy, plasma fibrinogen and other pro-coagulant factors increase, and they stay elevated until 4 to 6 weeks following delivery.
Now, there are some complications that can happen during the postpartum period, the main one being postpartum hemorrhage, meaning excessive blood loss following delivery. Other common complications include injuries to the genital tract, such as hematomas and lacerations. Hematomas are localized collections of blood that commonly affect the vulva, vagina, and perineum. They can cause significant pain and discomfort, and large hematomas can cause hemodynamic instability and even hypovolemic shock.
Lacerations, on the other hand, can affect the uterus, cervix, vagina and the perineum. Perineal lacerations can be classified in 4 degrees. First degree lacerations are when the tear doesn’t go past the fourchette, which is where the two labia minora meet posteriorly. Second degree lacerations extend past the fourchette, but they don’t involve the anal sphincter. Third degree lacerations may extend as far as the internal anal sphincter. Finally, fourth degree lacerations reach all the way to the rectal mucosa.
Next up, there are thromboembolic complications, like deep vein thrombosis, which is when a blood clot develops in one of the major veins, typically those of the lower leg. This clot can then break off and get lodged in other vessels, which can cause potentially life-threatening complications like a pulmonary embolism.
Now, infections can also occur during the postpartum period, and typically they only cause a fever, malaise and possibly tachycardia. However, left untreated, the infection can progress to potentially life-threatening septic shock or disseminated intravascular coagulation.
Up next, there are placenta-related complications, like retained placenta, which is when the placental delivery takes more than 30 minutes; and placenta accreta, which is a type of retained placenta, where the placenta grows into the uterine wall, and can’t be removed manually. The main problem with these conditions is that they can cause severe postpartum hemorrhage which can progress to hypovolemic shock.
Finally, it’s worth mentioning that some hypertensive disorders of pregnancy, like preeclampsia and eclampsia, can also debut in the postpartum period.
Some common risk factors for developing postpartum complications include extremes of age, like teenage pregnancy, or age over 35; grand multiparity, meaning 5 or more previous deliveries; uterine overdistention, like with multiple gestation or polyhydramnios; preterm delivery and premature rupture of membranes; using certain medications, like tocolytics or oxytocin; previous uterine surgery, like a previous cesarean birth; or use of operative procedures during delivery, like cesarean birth, vacuum extraction and forceps use. Postpartum complications also tend to be more common in individuals with preexisting health conditions, like diabetes or heart disease.
Each of these complications has its own clinical manifestations. Clients with vaginal or vulvar hematomas typically present with deep, severe pain and feelings of pressure that are not relieved by the usual pain-relief options. There can be intermittent bleeding, painful or difficult voiding, or emptying their bladder, as well as discolored, tender swelling over and around the hematoma.
Uterine lacerations typically cause excessive uterine bleeding that continues even when the fundus contracts firmly; whereas vaginal and perineal lacerations typically cause bleeding, pain and difficulty voiding.
With thromboembolic complications, most often there is a swollen, red, and painful lower leg; while a pulmonary embolism can cause dyspnea, cough or hemoptysis. Infections typically present with fever and tachycardia, and there could be foul smelling vaginal discharge. Next, the main clinical findings with retained placenta include excessive bleeding and an inability of the uterus to contract.
The diagnosis of postpartum complications starts with the client’s history and physical examination. Common lab tests include a CBC, which can show low hemoglobin and hematocrit in case of hemorrhage; or high WBC count, with an infection. Inflammatory markers, like CRP and ESR can also be elevated with an infection. A coagulation panel can also be done to look for abnormalities when suspecting a thromboembolic event. Imaging studies, like a pelvic ultrasound, can help identify placental complications; while a CT scan of the chest can help identify or rule out a pulmonary embolism.