Birth-related procedures: Nursing
Notes
| BIRTH-RELATED PROCEDURES | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| LABOR INDUCTION & AUGMENTATION |
| |
| ASSISTED VAGINAL DELIVERY |
| |
| EPISIOTOMY |
| |
Transcript
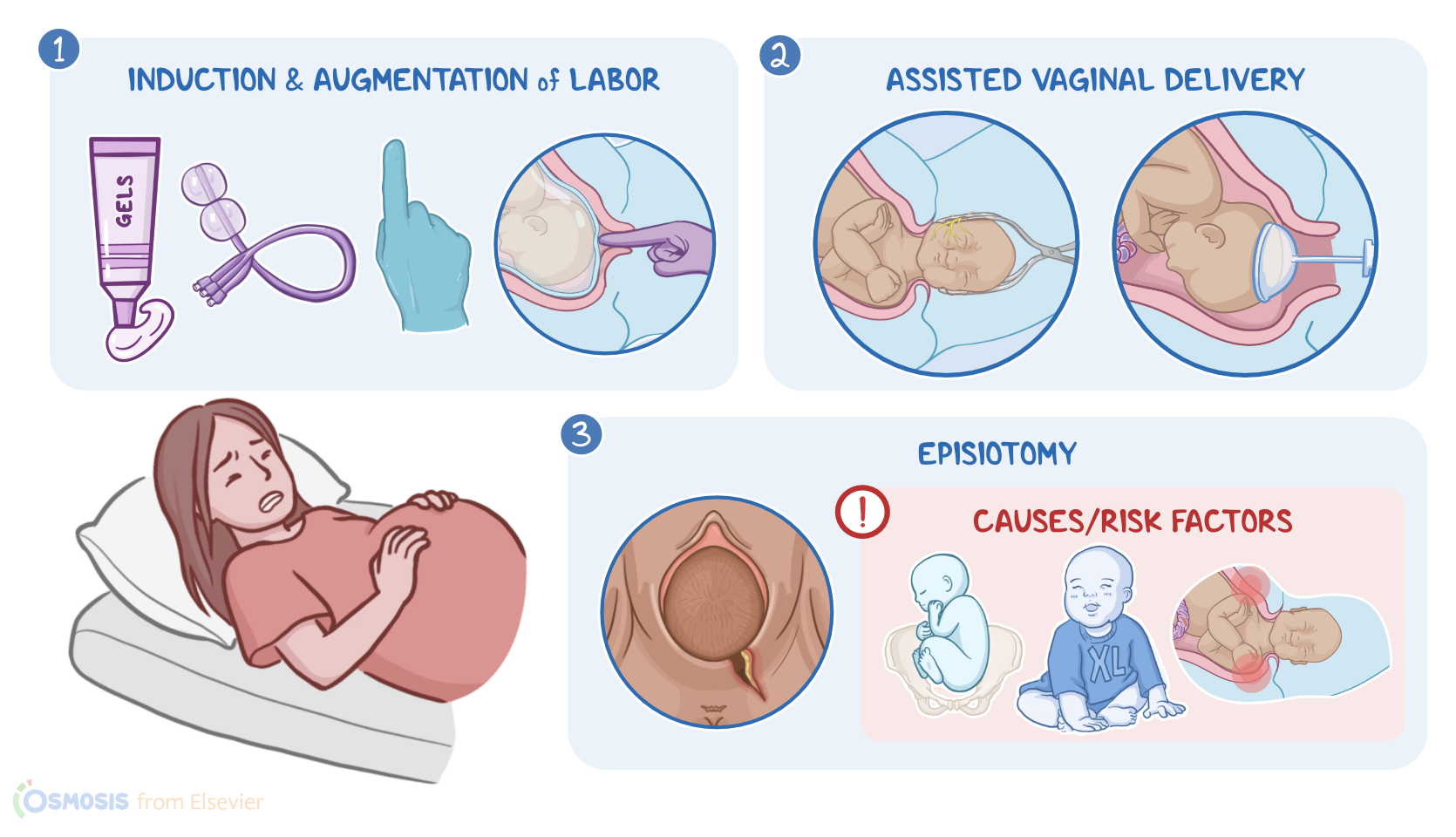
Labor, also called childbirth, is a physiologic process during which the fetus and placenta are expelled from the uterus. The most common form of delivery is vaginal, meaning that the baby passes through the vaginal canal. However, some deliveries require the assistance of healthcare providers in the form of birth-related procedures. These procedures include, labor induction and augmentation, assisted vaginal delivery, sometimes called operative vaginal delivery, and episiotomy.
Now, let’s discuss induction and augmentation of labor, which are artificial methods that start the labor process. One method is cervical ripening, which is used to ripen or soften the cervix so that it’s more likely to dilate with uterine contractions. Cervical ripening can be done pharmacologically or mechanically.
With pharmacological cervical ripening, prostaglandin E2, also known as dinoprostone, is most commonly used. It comes in the form of intravaginal gel, intracervical gel, or timed-release vaginal insert. Prostaglandin E1, also known as misoprostol, can also be used for cervical ripening, but it’s an off-label use. One setback of using prostaglandins for cervical ripening is that it also increases the contractility of the uterus, and can even result in tachysystole, or excessively frequent uterine contractions, so both the uterine activity and the fetal heart rate must be monitored when prostaglandin E2 is in place. When it comes to contraindications of cervical ripening, these include previous cesarean birth and major uterine surgery.
For mechanical cervical opening, there are two methods. The first can be done using a trans-cervical balloon catheter. A trans-cervical catheter is inserted through the internal cervical os, or cervical opening, and the balloon is inflated. Then, the balloon is retracted down against the cervical os. This creates direct pressure and induces release of endogenous prostaglandins.
On the other hand, membrane stripping involves the digital separation of the amniotic membrane from the cervical and uterine walls.