Candidiasis: Nursing process (ADPIE)
Notes
| CANDIDIASIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
27-year-old Olivia Hartman presents to the gynecology clinic with complaints of vulvar itching, white, clumpy vaginal discharge, and painful intercourse. She reports that she recently completed antibiotic therapy to treat an urinary tract infection. After a sample of the vaginal discharge is tested, the gynecologist diagnoses Olivia with candidiasis and antifungal treatment is prescribed.
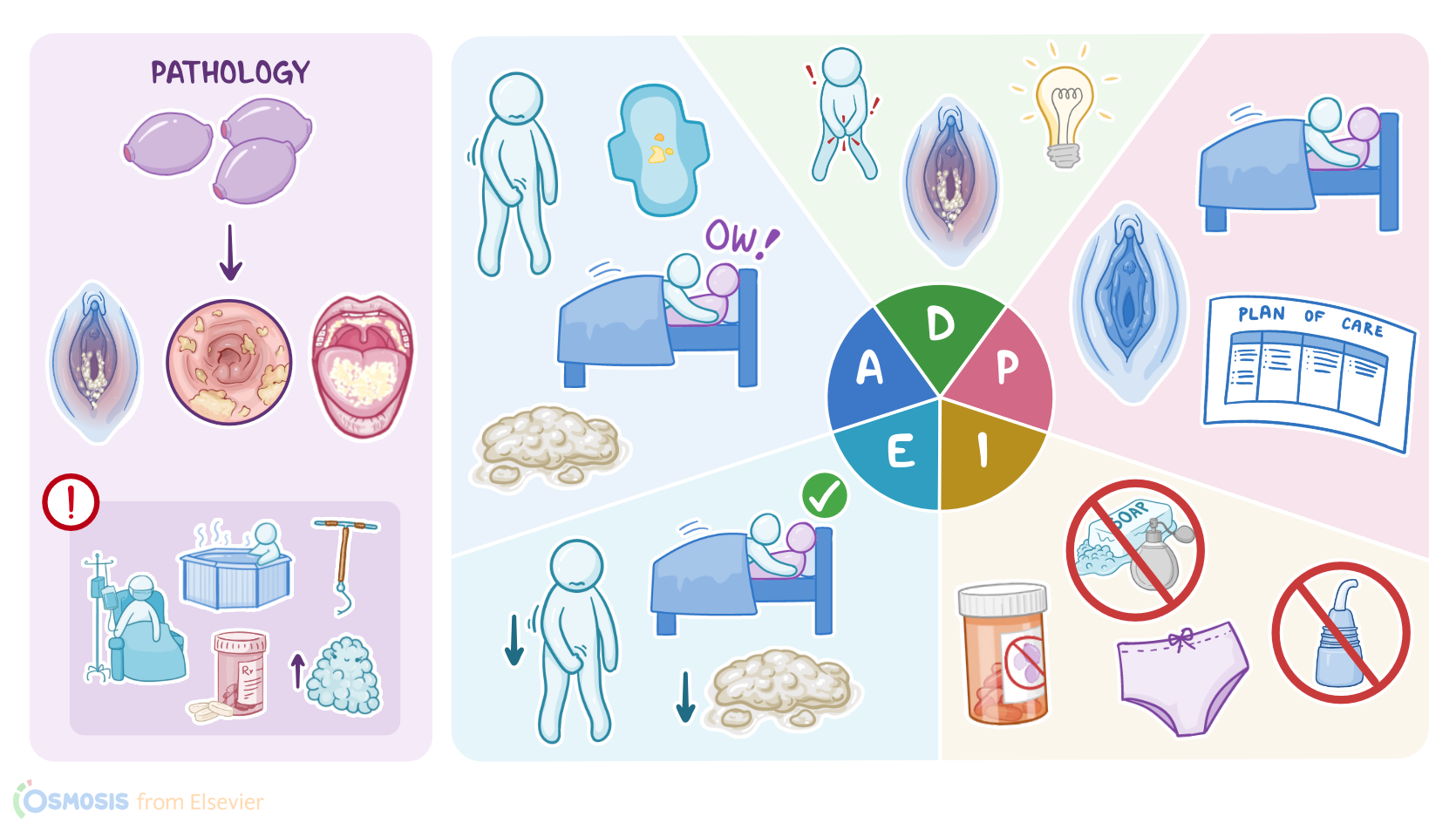
Now, candidiasis is a fungal infection caused by Candida species, most commonly Candida albicans. Candida albicans makes part of the normal human microbial flora, so it’s typically present in low numbers on the skin and mucous membranes, most notably the vaginal mucosa in females. Now, candidiasis occurs when there’s overgrowth of Candida albicans which disrupts the normal microbial flora. Most often, candidiasis affects the female reproductive organs, therefore it’s often referred to as candida vulvovaginitis. However, other frequent locations for Candida infection include the mouth, esophagus, and moist and warm areas of the skin, like groins or armpits.
One of the most common risk factors for Candida overgrowth is recent antibiotic use, since it kills off some important bacteria that are also part of the normal microbial flora, which means that there’s normally less competition for Candida to thrive. Other important risk factors include having diabetes mellitus, being immunocompromised, or taking corticosteroids, all of which can lead to a weakened immune system that can’t keep Candida under control. Finally, there’s increased risk of candidiasis in those who use hot tubs, as well as those with intrauterine devices, implanted prosthetic devices or high estrogen levels, which can be due to combined oral contraceptive use, estrogen therapy, or pregnancy, since all these factors favor Candida overgrowth.
The most important clinical feature of candidiasis is a thick, white, odorless vaginal discharge, that looks like cottage cheese. Additionally, clients can present with local erythema, edema, and excoriation of the vulva, associated with vulvar itching and burning, as well as dyspareunia, or painful intercourse, and dysuria, or painful urination. Unfortunately, many clients can experience recurrent candidiasis, which is defined as four more episodes of candidiasis within one year. Now, in immunocompromised clients or those with implanted prosthetic devices, Candida may get into the blood, causing candidemia. From the blood, Candida can spread to other organs, which is known as invasive candidiasis.
Diagnosis is based on clinical findings and potassium hydroxide, or KOH test, in which a sample of the vaginal discharge is mixed with 10% potassium hydroxide, eventually revealing signs of Candida infection like budding yeasts, hyphae, and pseudohyphae. If the KOH test is negative, a vaginal culture is needed to confirm the diagnosis. Finally, clients with candidiasis typically have a normal vaginal pH, which is between 4.0 and 4.5, which helps rule out other causes of vaginosis. Finally, diagnosis of candidemia or invasive candidiasis is done by taking a blood or tissue sample and sending it for culture.
Treatment of candidiasis can involve topical or oral antifungal medications like azoles. The preferred treatment is generally a single dose of oral fluconazole. Finally, all clients should have good body hygiene and avoid excess moisture.
Now, let’s see how Olivia is doing. After washing your hands, introducing yourself, and confirming Olivia’s identity, you begin your assessment. When you ask about her symptoms, Olivia reports persistent itching on and around her vulva and increased vaginal discharge. You assess the affected area and note that her vulva is edematous with localized erythema. You observe active vaginal discharge that resembles cottage cheese and is odorless. Olivia tells you that she is sexually active with her spouse, but stopped having intercourse when it became uncomfortable. She expresses concern about possibly infecting her husband, and wonders if he will need treatment too. You assure Olivia that candidiasis is not considered a sexually transmitted infection and her husband should remain unaffected. Her vital signs are: temperature 98.6 F or 37 C, heart rate 70 beats per minute, respirations 16 per minute, blood pressure 113/60 mmHg, and oxygen saturation 99% on room air. You document your findings and leave the room to confer with the gynecologist.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Treatment for recurrent vulvovaginal candidiasis (thrush)" Cochrane Database Syst Rev (2022)
- "Invasive Candidiasis" Semin Respir Crit Care Med (2020)
- "Pathogenesis and virulence of Candida albicans" Virulence (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Candidemia and Invasive Candidiasis" Infect Dis Clin North Am (2021)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)