Contraception - Hormonal methods: Nursing
Notes
| CONTRACEPTION - HORMONAL METHODS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| HORMONAL CONTRACEPTIVES |
| |
| PROGESTIN-ONLY CONTRACEPTIVES |
| |
| COMBINED ORAL CONTRACEPTIVE PILLS |
| |
| TRANSDERMAL PATCHES AND VAGINAL RINGS |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
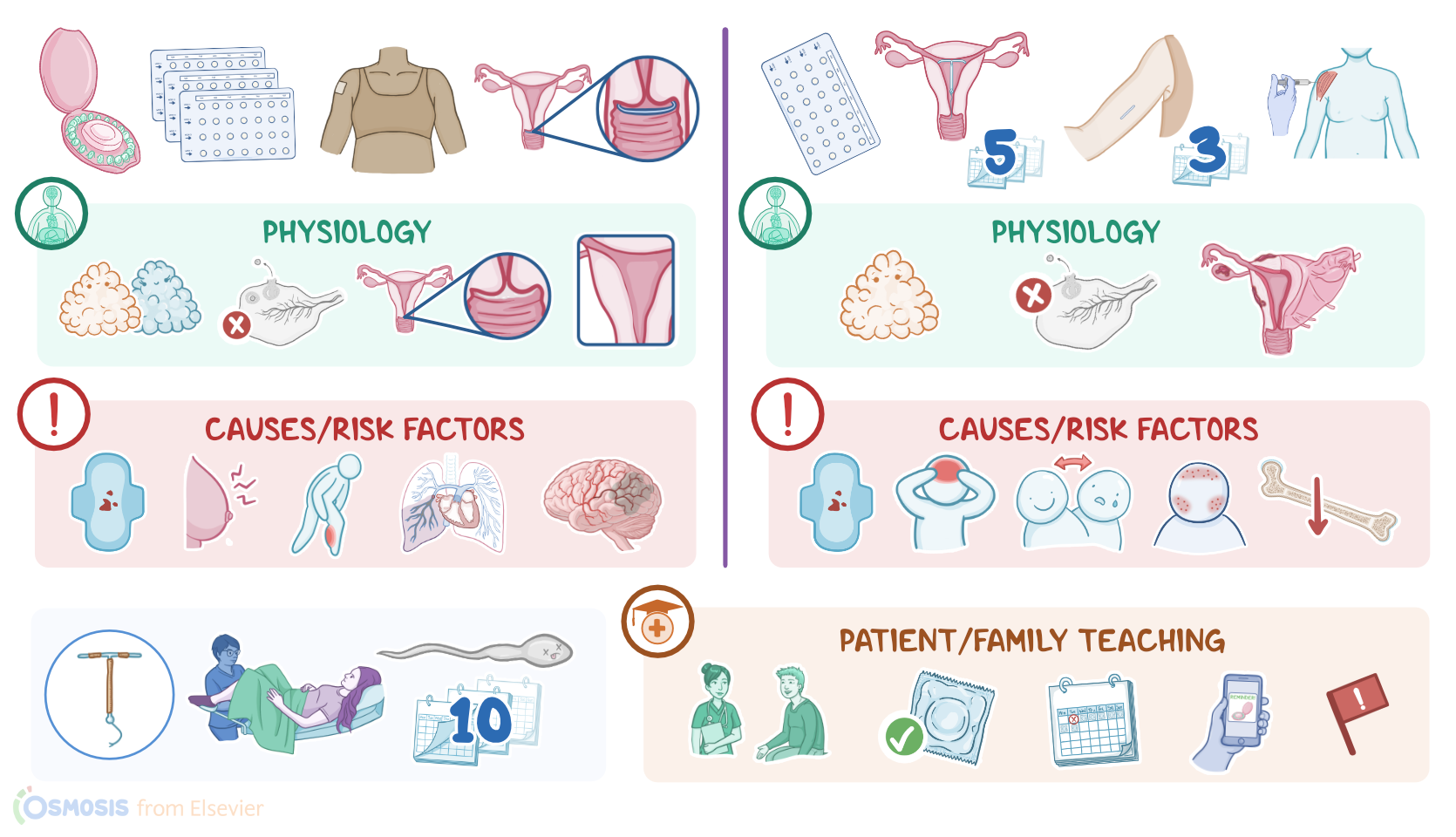
Contraception or birth control refers to various methods that prevent pregnancy, and they can range from devices to medications and different procedures. Hormonal methods are some of the most popular means of contraception that can be used. They contain different concentrations of estrogen and progestin or sometimes progestin alone and are available as pills, injections, combined oral pills, vaginal rings, skin patches, as well as subcutaneous or intrauterine implants.
Now, to understand hormonal methods of contraception, let’s start by having a look at the ovaries, which are the gamete and hormone producing organs in individuals assigned female at birth. The ovaries contain ovarian follicles, which house the female gametes, called oocytes. Ovarian follicles also secrete the hormones estrogen and progesterone, which have a key role in the menstrual cycle and ovulation. Hormone production, as well as ovulation, which refers to the release of an oocyte each month, is under the control of the hypothalamus and the pituitary gland, way up in the brain.
See, the hypothalamus secretes gonadotropin releasing hormone, or GnRH, which tells the pituitary to secrete follicle-stimulating hormone, or FSH, and luteinizing hormone, or LH. FSH stimulates the maturation of a dominant ovarian follicle each month during the follicular phase of the menstrual cycle, which goes from the first day of menstruation until day 14 of an average 28 day cycle. As the dominant follicle matures, it secretes more and more estrogen, which acts as a negative feedback signal, meaning it tells the pituitary to secrete less FSH, as well as LH, since there’s so much estrogen around. That is how it goes until day 14, which is when ovulation occurs.
Now, right before ovulation, estrogen levels increase past a critical point, and they become a positive feedback signal. This basically translates to the pituitary as enough estrogen has been produced for ovulation to occur. In turn, the pituitary secretes a surge of FSH and LH, which causes the ovarian follicle to rupture and release the oocyte in the fallopian tube, where it can be fertilized by a sperm.
After ovulation, comes the luteal phase of the menstrual cycle, which lasts from day 15 to day 28 of an average 28 day cycle. During this phase, the remains of the ovarian follicle become the corpus luteum, which secretes progesterone that thickens the endometrial layer, to get it ready for implantation of a potentially fertilized egg. Progesterone also acts as a negative feedback signal for LH, preventing a second ovulation in the same month. Now, if fertilization doesn’t occur, the corpus luteum degenerates, and progesterone levels decrease. This causes the innermost layer of the uterus, called the endometrium, to slough off, which starts menstruation and a brand new menstrual cycle.
For fertilization and pregnancy to occur, on the other hand, sperm must reach the oocyte. This commonly happens during intercourse when the penis releases the sperm into the vagina. From there, the sperm cross the cervix and the uterine cavity, to finally reach the fallopian tube, where one of them can fertilize the oocyte, so that a zygote is formed. The zygote then starts dividing and travels back to the uterine cavity, where it implants; and so pregnancy starts.
With that in mind, let’s go through the various methods of hormonal contraception. Of note, while all of these methods are highly effective contraceptives when used correctly, none of them prevent against sexually transmitted infections, like condoms do.
Let’s start with progestin-only contraceptives. They prevent pregnancy mainly by inhibiting pituitary LH secretion, therefore preventing ovulation. Additional contraceptive mechanisms include thickening the cervical mucus so sperm can’t get through, and thinning of the endometrial lining so implantation can’t occur. In this way, they can often cause amenorrhea.
In cases where they don’t cause amenorrhea, they can lessen the pain and blood loss during menstruation. So they may be useful for clients who have significant dysmenorrhea or excessive blood loss during their periods, like those with endometriosis. There are some progestin-related side effects, which may include breakthrough bleeding, spotting, headaches, nausea, weight gain, mood swings, breast tenderness, and acne.
Now, progestin-only contraceptives are available as oral pills, IUDs or intrauterine devices, implants, and injections. The progestin-only pills, also called mini pills, are taken orally on a daily basis, and they should be taken at the same hour each day for maximum contraceptive effectiveness. With a slight increase in the dosage, they can also be used as emergency contraceptive or “morning after” pill that can be effective as long as it’s taken within 72 hours after sex. However, they are ineffective if the zygote implantation has already occurred.
Next, IUDs are inserted through the vagina into the uterus by clinicians, between days 1 and 5 of the menstrual cycle, in which case the contraceptive effect is immediate. If inserted later than day 5 of the menstrual cycle, back-up contraception, like condoms, should be used for about 7 days, until the contraceptive effect of the IUD kicks in. Besides progestin-only IUDs, there are also non-hormonal, or copper IUDs, also called Copper Ts, which work because copper creates a spermicidal environment inside the uterus. Unlike progestin-only IUDs, the Copper T can be inserted on any day of the menstrual cycle, and the contraceptive effect is immediate.
Next up, there are progestin-only implants, that can be inserted subcutaneously, under the skin of the upper arm. The procedure is painless thanks to local anesthesia, and the device releases systemic progestin continuously to provide contraception for 3 years.
Lastly, a progestin-only injection containing medroxyprogesterone acetate is administered intramuscularly every 3 months, and can prevent ovulation up to 15 weeks. Although very safe, in some occasions progestin-only contraceptives can increase the risk of follicular ovarian cysts and weight gain in some clients. With long term use, they may cause loss of bone mineral density.
Sources
- "Medical-Surgical Nursing" Elsevier (2020)
- "Foundations of Maternal-Newborn and Women's Health Nursing" Saunders (2018)
- "Study Guide for the Core Curriculum for Oncology Nursing" Saunders (2019)
- "Medical-Surgical Nursing" Mosby (2019)
- "Contemporary Hormonal Contraception and the Risk of Breast Cancer" New England Journal of Medicine (2017)
- "Hormonal Contraception and Bone Health in Adolescents" Frontiers in Endocrinology (2020)
- "Contraception options and provision to adolescents" Minerva Pediatrics (2017)
- "Contraception" Endotext (2018)