Cholelithiasis: Nursing
Cholelithiasis: Nursing
Gastrointestinal System
Gastrointestinal System
Notes
| CHOLELITHIASIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
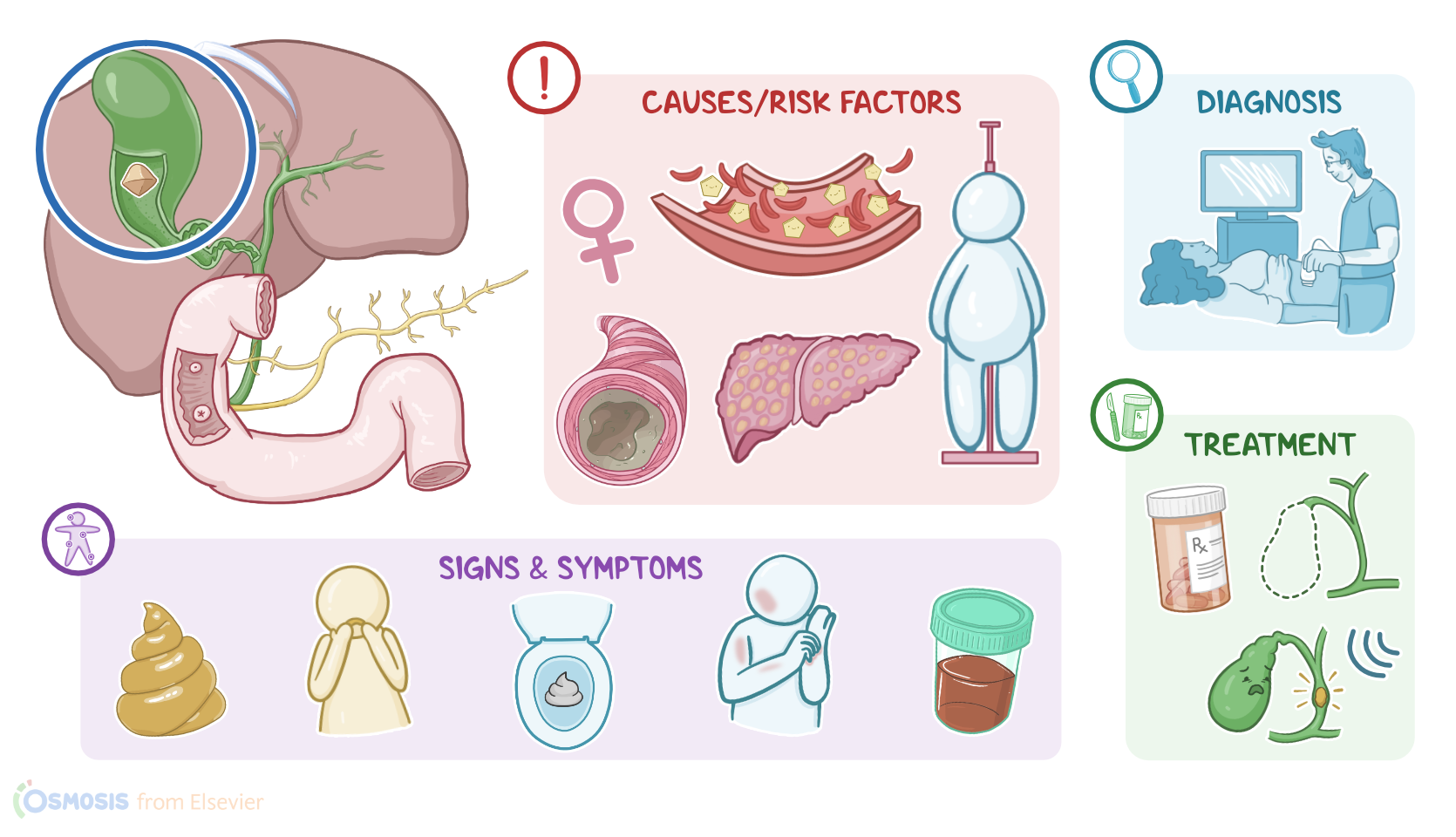
Cholelithiasis refers to the presence of gallstones, or calculi, in the gallbladder as a result of precipitation of bile components, such as cholesterol and bilirubin.
Now, let’s quickly review some anatomy and physiology of the hepatobiliary system, which is made of the liver, gallbladder, and bile ducts. The liver is in charge of producing bile, which is mostly made up of bile salts and acids, cholesterol, phospholipids, proteins, bilirubin and small amounts of various other compounds, like water, electrolytes, and bicarbonate.
Then, bile flows out of the liver through the hepatic ducts towards the gallbladder, where it’s stored. Now, eating fatty foods stimulates the cells in the small intestine to secrete cholecystokinin into the bloodstream.
Cholecystokinin, in turn, stimulates the gallbladder contraction, causing it to release bile through the cystic duct, then the common bile duct, and ultimately into the duodenum. Once in the duodenum, bile acts as a fat emulsifier, which essentially helps to digest lipids from food into small micelles, making them easier to absorb.
Now, gallstone formation is caused by precipitation of bile components, such as cholesterol and bilirubin, respectively leading to the formation of cholesterol gallstones and pigment gallstones.
That being said, the main risk factors for cholesterol gallstones include being assigned female at birth, pregnancy, and oral contraceptive pills are associated with higher estrogen levels, which then increases cholesterol synthesis in the liver. Other common risk factors include obesity and a high cholesterol diet; as well as increasing age, especially after 40. These can be remembered by the 3 Os for stooones, so ovulating, obesity, and older.
Next, anything affecting the terminal ileum, like Crohn’s disease, or ileal resection, can reduce the reabsorption of bile acids into the circulation and back to the liver, increasing the risk of cholelithiasis. In addition, gallbladder stasis, or inactivity, has also been linked to gallstone formation. Risk factors for that include pregnancy and oral contraceptives, since progesterone also slows gallbladder emptying; and prolonged parenteral nutrition, which decreases cholecystokinin release and leads to biliary stasis.
On the other hand, risk factors for pigment gallstones include conditions that cause extravascular hemolysis, such as sickle cell anemia. In these situations, an increased rate of red blood cells metabolism leads to higher levels of bilirubin in the blood, which then passes on to the biliary tract. Other risk factors include conditions like cirrhosis, and cystic fibrosis.
Alright so, cholesterol gallstones are formed when the bile becomes supersaturated with cholesterol. This means that there’s so much cholesterol that the bile salts and phospholipids can’t hold anymore in solution. As a result, cholesterol precipitates, forming solid cholesterol monohydrate crystals.
In addition to cholesterol supersaturation, there’s biliary stasis due to mucus hypomotility, and hypersecretion in the gallbladder. In this environment, more cholesterol is added to existing crystals, leading to the formation of gallstones.
On the other hand, pigment gallstones are formed when there’s a concentration of unconjugated bilirubin in the bile that is higher than normal. These will bind to calcium ions and precipitate into calcium bilirubinate.
Now, these gallstones can either remain in the gallbladder, or move out and get lodged in a duct along their way, obstructing its bile flow. If the gallstone obstructs the cystic duct, this can lead to serious complications like acute cholecystitis, or inflammation of the gallbladder due to bile buildup. If the gallstone gets lodged further down in the common bile duct, this also blocks the flow of bile from the liver, which is known as cholestasis.