Cleft lip and palate: Nursing
Introduction0:00–0:18
Cleft lip is an opening or a split in the upper lip, whereas cleft palate describes an opening or a split in the roof of the mouth, called the hard palate.
Cleft lip and palate are the most common congenital anomalies of the head and face.Now, let’s quickly review the embryological development of the lips and palate.
Physiology0:18–1:33
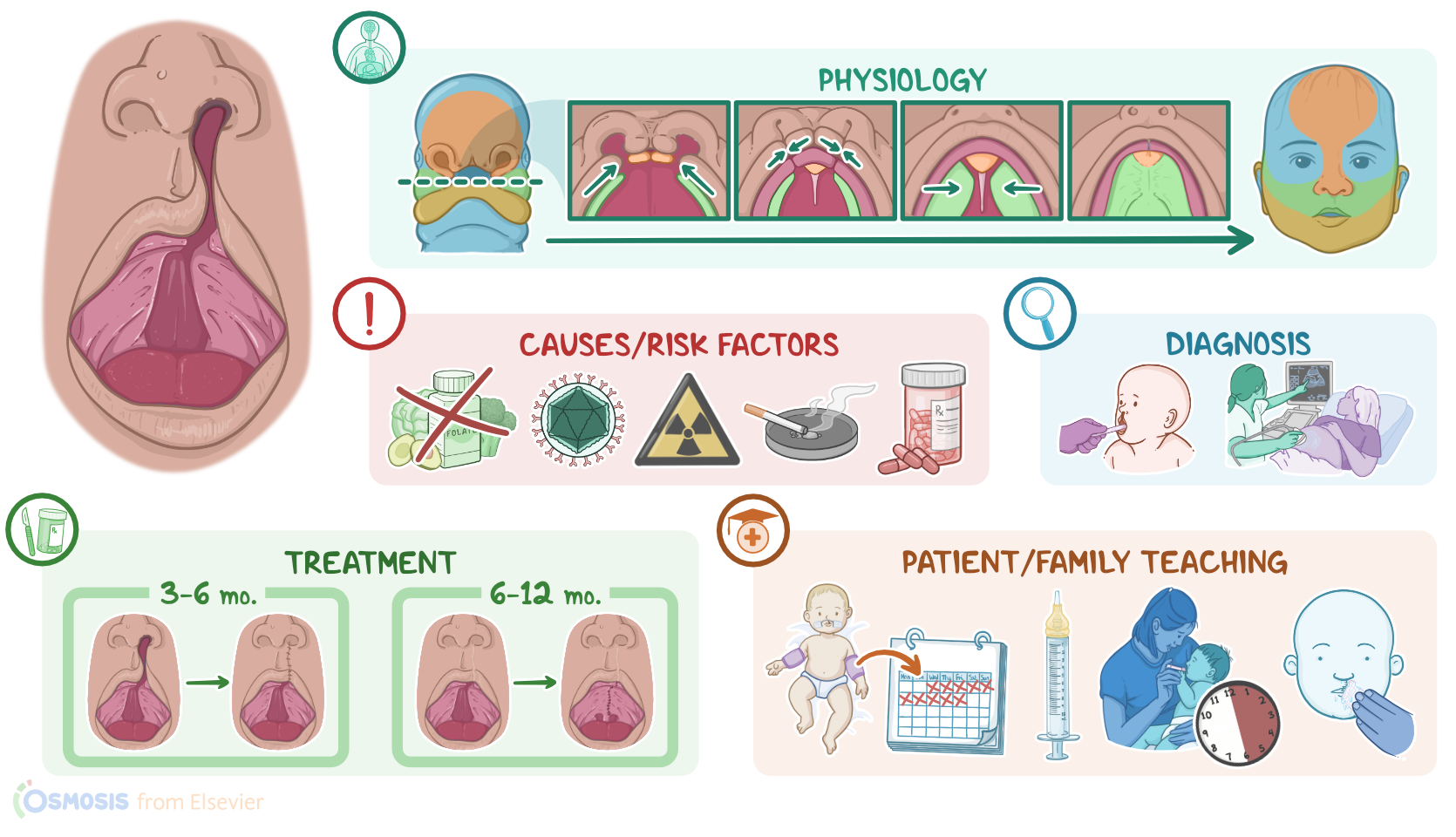
At the fourth week of pregnancy, multiple structures appear in the face of the embryo. These include the frontonasal prominence, which gives rise to the forehead and bridge of the nose; nasal placodes, which are two raised bumps on each side of the frontonasal prominence; as well as paired maxillary prominences; and paired mandibular prominences.
Additionally, two small dimples develop at the center of each nasal placode, dividing these placodes into medial and lateral nasal prominences.Now let’s look at a cross section of the embryo.
As the embryo develops, the maxillary prominences grow medially to fuse with the medial nasal placodes, giving rise to the upper lip.
In addition, the medial nasal placodes grow to the inside of the face, forming the intermaxillary segment, which later on forms the anterior one third of the hard palate, called the primary palate.
Similarly, the maxillary prominences grow to the inside of the face, forming the palatal shelves. These shelves will then fuse above the tongue to form the remaining two thirds of the hard palate, called the secondary palate.Alright, now the cause of cleft lip and palate is unknown, with some theories suggesting multifactorial genetic and environmental involvement.
Causes & risk factors1:33–2:08
However, several risk factors for cleft lip and palate have been identified, including folate deficiency, as well as exposure to teratogens, such as maternal smoking and exposure to radiation, and using certain medications during pregnancy, such as anticonvulsants or steroids.
Other risk factors include advanced maternal age, and certain infections during pregnancy, especially the rubella virus.Moving on to pathology and starting with cleft lip, the maxillary prominences fail to fuse with the medial nasal prominences at the midline, causing a split in the upper lip.
Pathology and complications2:08–2:49
On the other hand, a cleft palate occurs when the palatal shelves fail to fuse at the midline.When it comes to complications of cleft lip and palate, these include feeding difficulties, which can lead to insufficient growth; as well as altered dentition; delayed or altered speech development; and recurrent otitis media that can progress to hearing loss.
Other complications are often caused by a cleft palate, and these include gagging, choking, and nasal regurgitation of milk.
Clinical manifestations2:49–3:25
Clients with cleft lip and palate typically present with a split in the upper lip or a split in the roof of the mouth. A cleft lip can present without a cleft palate, and vice versa, with up to 50 percent of clients presenting with both defects.
These defects can be bilateral, meaning on both sides, or unilateral, meaning on one side only, with the left side being more commonly affected.
Other signs and symptoms include a split in the upper lip that extends to one or both nostrils; or a split in the hard palate that doesn’t affect the face.
The diagnosis of cleft lip and palate is based on physical assessment of the newborn, and can also be done prenatally via routine ultrasound.The mainstay of treating cleft lip and palate is surgery, which aims at improving the child’s ability to eat, speak, and hear normally, in addition to restoring normal facial appearance.
Diagnosis3:25–3:34
Treatment3:34–4:01
Surgical repair of cleft lip, or cheiloplasty, usually occurs between 3 and 6 months of age. Surgical repair of cleft palate, or palatoplasty, is corrected with a series of surgeries.
The initial surgery usually occurs between 6 and 12 months of age.Alright, now let’s look at the nursing care you’ll provide to an infant with a cleft lip.
Management of care4:01–5:18
Your primary nursing goals are to provide postoperative care and provide emotional support.Okay, begin by implementing routine postoperative interventions, and monitor the infant closely for complications related to the procedure.
To help decrease the risk of damaging the surgical site, apply soft elbow immobilizers that allow movement, but prevent the infant from bending their arm at the elbow to reach the suture line.
Also maintain the curved metal protective device called a Logan bow, to provide additional protection and to decrease stress on the surgical site.When the infant is able to tolerate oral nutrition, provide small feedings through an oropharyngeal syringe or other special feeder.
Also, be sure to position them in an upright position during and at least 30 minutes after each feeding to help prevent aspiration, and use clear water to gently rinse the mouth and suture line to help prevent infection.Finally, support the caregivers by providing emotional and psychological support.
Encourage caregivers to participate in care; and be sure to use active listening; allow plenty of time for them to ask questions, and give clear, concise answers.Okay, let’s move on to client and family teaching.
General client & family teaching5:18–6:14
Begin by explaining how a cleft lip occurs, and the procedure for correcting the defect. Review the plan of care, instruct them to administer the prescribed medications exactly as directed, & underscore the importance of keeping all of the follow-up appointments with their baby’s healthcare provider for continued monitoring and care.Next, teach them how to feed their baby with the prescribed syringe, and let them know that after the incision has fully healed, their baby can resume breast or bottle feeding.
Teach them how to care for the incision site, and explain that the elbow restraints should remain in place for 10 days postoperatively.Explain that a small amount of drainage is normal, but they should contact their healthcare provider if there’s redness, swelling, bleeding, bad-smelling drainage, or increased pain around their surgical incision.Alright, as a quick recap… Cleft lip is an opening or split in the upper lip; and cleft palate is an opening or split in the hard palate.Now, normally during the fourth week of development, the embryo develops the frontonasal prominence, nasal placodes, paired maxillary prominences, and the paired mandibular prominences, and eventually fuse together forming the primary and secondary palate.The cause of cleft lip and palate is unknown but theories suggest multifactorial genetic and environmental components.
Review6:14–7:42
Risk factors include advanced maternal age; folate deficiency; maternal smoking or exposure to radiation; use of medications, like anticonvulsants or steroids; and certain infections during pregnancy.As for pathology, a cleft lip is formed when the maxillary prominences fail to fuse with the medial nasal prominences at the midline, causing a split in the upper lip.
A cleft palate occurs when the palatal shelves fail to fuse at the midline.Diagnosis is based on the physical assessment of the newborn.
The main treatment is surgical repair. Your priority goals of care are to provide postoperative care and provide emotional support.
Client and family teaching is focused on strategies for caring for the child at home and when to contact the healthcare provider.
| CLEFT LIP AND PALATE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
- "Medical-Surgical Nursing" Elsevier (2020)
- "Lewis's Medical-Surgical Nursing" Mosby (2019)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Saunders (2016)
- "Maternal Child Nursing Care" Elsevier Health Sciences (2014)
- "Essentials of Pediatric Nursing" LWW (2020)
- "Prenatal diagnosis of cleft lip and cleft lip palate – a case series" Medical Ultrasonography (2018)
- "State-Mandated Coverage of Cleft Lip and Cleft Palate Treatment" The Cleft Palate-Craniofacial Journal (2020)
- "Regulatory Mechanisms of Soft Palate Development and Malformations" Journal of Dental Research (2019)
- "Cleft lip and palate: Care configuration, national registration, and research strategies" Journal of the World Federation of Orthodontists (2020)
No notes for this video yet
Try adding a note below