Conjunctivitis: Nursing process (ADPIE)
Conjunctivitis: Nursing process (ADPIE)
FINAL
FINAL
Notes
| CONJUNCTIVITIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
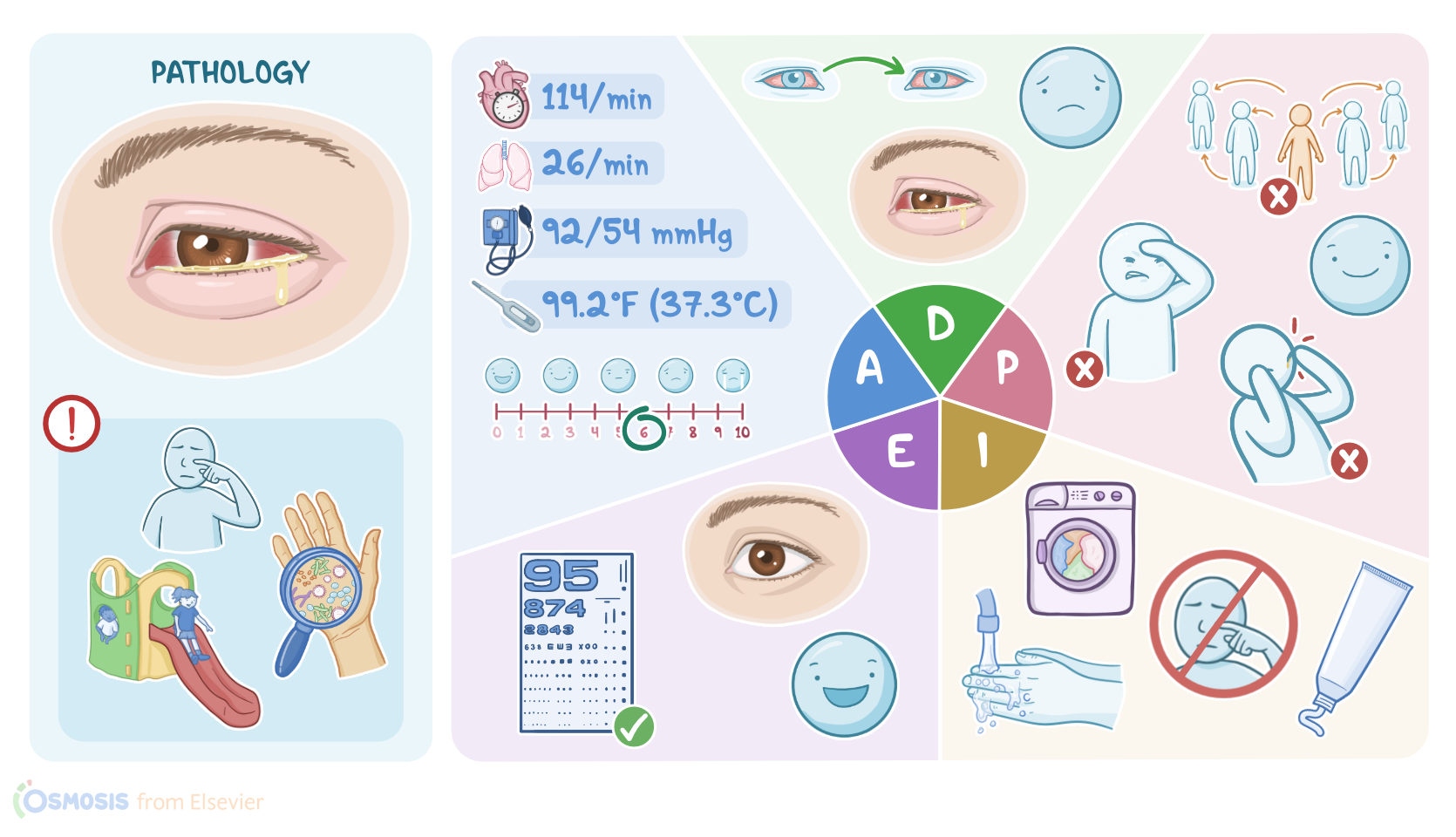
Leilani Flores is a 3-year-old client who was brought to the primary care clinic by her father, Alvin. Yesterday, Leilani’s older sister was diagnosed with bacterial conjunctivitis, and was started on antibiotic eye drops.
Today, Alvin is concerned that the infection has spread to Leilani. He reports that she woke up with her right eye crusted shut with yellow drainage and she has been rubbing the eye frequently.
Conjunctivitis, commonly known as pink eye, refers to the inflammation of the conjunctiva, which is the clear membrane that covers the sclera and the inner surface of the eyelids, in response to an infection, allergen, or irritant.
As a result there’s dilation of conjunctival blood vessels, which typically causes the eye to look pink or red. So, there are two main causes of conjunctivitis, infectious and non-infectious.
Infectious conjunctivitis can be further divided into viral and bacterial conjunctivitis. Viral conjunctivitis is the most common one and is typically caused by adenovirus, but can be also due to herpes simplex virus or varicella-zoster virus.
On the other hand, bacterial conjunctivitis is most often caused by Staphylococcus Aureus, Streptococcus pneumoniae, or Haemophilus influenzae, but less commonly, it can also be caused by Neisseria gonorrhoeae, or Chlamydia trachomatis.
Both viral and bacterial conjunctivitis are highly contagious, and spread through direct hand-to-eye contact with contaminated objects, or with an infected person’s secretions like tears or eye discharge.
So, the main risk factors include close contact with someone who has conjunctivitis, as well as attending crowded places like schools or daycare.
Other factors that increase the risk of conjunctivitis include poor hand hygiene and improper use of contact lenses. There’s also non-infectious conjunctivitis, which includes allergic and irritant conjunctivitis.
Allergic conjunctivitis is usually caused by airborne allergens, like pollen, grass, or dust, and an important risk factor is the season, especially during spring.
On the other hand, irritant conjunctivitis can be caused by a mechanical irritant, such as a foreign body or chemical irritants found in smoke, fumes, powders, and liquids like chlorine or alcohol.
In terms of symptoms, conjunctivitis presents with unilateral or bilateral pink or red eyes, which can be associated with mild eyelid and conjunctival edema, as well as sensitivity to light, and excessive lacrimation.
In viral and non-infectious conjunctivitis, there’s watery discharge, while in bacterial conjunctivitis, the discharge is purulent, white, yellow, or green, and clients may often wake up with crusted or sticky eyelids.
For allergic conjunctivitis, a telltale sign is excessive eye itchiness, and it's usually associated with a runny nose or sneezing. Most cases of conjunctivitis are usually self-limited, but severe cases of infectious conjunctivitis can lead to complications if the infection spreads to other structures of the eye.
Some bacteria may penetrate further into the cornea, causing keratitis or corneal inflammation, and may ultimately result in corneal ulceration or even blindness.
Bacteria can also spread to the lacrimal sac, causing dacryocystitis. Now, diagnosis of conjunctivitis is usually clinical, based on history and physical examination.
For infectious conjunctivitis, laboratory tests of the eye discharge, such as rapid antigen detection tests for viruses, or gram stain and culture for bacteria might be necessary to detect the causative pathogen.
For treatment, viral conjunctivitis is typically self-resolving, but lubricant drops or ointments might help with symptoms. On the other hand, bacterial conjunctivitis generally requires antibiotic drops or ointments.
Additionally, applying warm and wet compresses can help clear the sticky discharge. Allergic conjunctivitis is usually treated with antihistamines, either orally or as eye drops, as well as by avoiding the allergen.
Finally, irritant conjunctivitis is usually self-resolving, but flushing the eyes, removing and avoiding the irritant, and applying lubricant eye drops can be helpful.
As you enter the room, you begin your assessment. Leilani's father, Alvin, is holding her in his lap and she appears irritable and uncomfortable. When you ask Leilani how her eye feels, she tells you “it itches and hurts.”
Sources
- "Conjunctivitis: A Systematic Review" J Ophthalmic Vis Res (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Viral Conjunctivitis" Viruses (2023)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Bacterial conjunctivitis" Visual Journal of Emergency Medicine (2023)
- "A Review of the Differential Diagnosis of Acute Infectious Conjunctivitis: Implications for Treatment and Management" Clin Ophthalmol (2020)