Enuresis: Nursing
Enuresis: Nursing
NUR243
NUR243
Notes
| ENURESIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Enuresis refers to involuntary urination in children who have passed the age of toilet training, which is typically around 5. Enuresis is more commonly known as “bedwetting,” and this is called nocturnal enuresis if it happens mainly at night, or diurnal enuresis if it mainly happens during the day. Primary enuresis is defined as involuntary urination in a client who has never developed bladder control. Secondary enuresis refers to involuntary urination in a client who’s already developed bladder control.
Okay, first, let’s cover some basic physiology of urine production and excretion. Kidneys filter the blood to produce urine in a process that is controlled by several hormones, including vasopressin, which is also known as antidiuretic hormone, or ADH for short. ADH is produced by the hypothalamus and stored in the posterior pituitary. Now, when a person is thirsty or dehydrated, the posterior pituitary releases ADH into the blood, which then travels to the kidneys to increase water reabsorption, subsequently decreasing urine production. More ADH is released during the night to prevent urination until the morning.
Now, once the kidneys filter the blood, they produce urine that is passed through ureters down into a hollow, muscular organ called the bladder. The bladder’s main function is to store urine, and as the urine accumulates, the walls of the bladder start to stretch, subsequently stretching the specialized nerve cells located in the bladder wall. Once stretched enough, these nerve cells send a signal through the spinal cord to the pontine micturition center in the brainstem and activates the micturition reflex. As a result, the bladder contracts to push out urine, while the internal and external urethral sphincters relax to let the urine out. Ultimately, this results in micturition or urination.
Now, until the 12th month of life, infants have no voluntary control over urination. Between the 12th and 18th month, they develop some control, while between the 24th and 30th month, most people develop full control over the bladder. Moreover, older children and adults can delay emptying their bladder if they are in a socially unacceptable situation. In these situations, the brain sends inhibitory signals to the pontine micturition center, eventually preventing the contraction of the bladder and micturition.
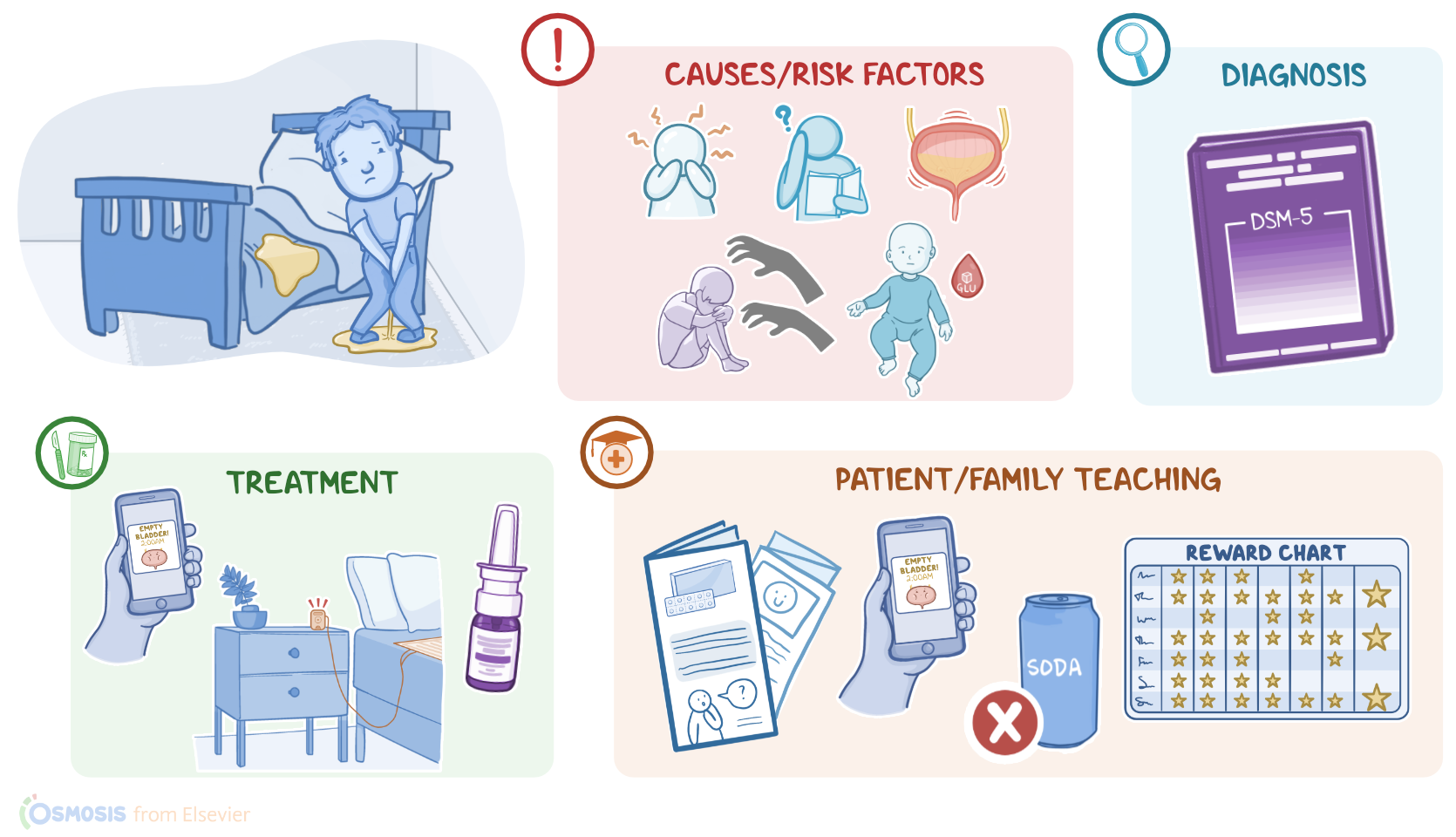
The exact cause of primary enuresis remains unknown, but some theories suggest that this condition could be associated with anxiety and neurodevelopmental problems, as well as slow maturation, or hyperactivity of the bladder. On the other hand, common causes of secondary enuresis include physiological stress, like sexual abuse; central diabetes insipidus; and medications, such as valproate, which is used to treat epilepsy in children. Other causes of secondary enuresis include urinary tract infections and constipation.
Now, important risk factors for developing enuresis include a family history of enuresis; low socioeconomic status; and major life changes or stressors, like the birth of a sibling, family conflict, or separation from a parent or guardian.
Now, the exact pathological process of primary enuresis remains unclear, but some sources suggest that three factors contribute to the development of primary nocturnal enuresis. The first factor is decreased ADH production, especially at night. This results in decreased water reabsorption and subsequently increased urine production when the person is sleeping. Next, there’s reduced functional capacity of the bladder, which means the bladder can store less urine before micturition is triggered. Finally, there’s the inability to wake up when the bladder is full. Often, it’s a combination of these 3 factors that leads to nocturnal enuresis.
Now moving on to the pathology of secondary enuresis, starting with central diabetes insipidus, which is also associated with decreased production of ADH by the hypothalamus. Next up is the use of valproate. One theory suggests that valproate can trigger the thirst center and increase water intake, eventually increasing urine production. The second theory suggests that valproate can cause bladder contraction and relaxation of the urinary sphincters.. Similarly, urinary tract infections, like cystitis, or inflammation of the bladder, can induce uncoordinated contractions of the bladder that can result in enuresis. Finally, enuresis can be caused by constipation, because the rectum fills with stool and directly exerts pressure on the surrounding structures, including the urethral sphincters, the bladder, and the nerves that innervates them. Moreover, this expansion of the rectum decreases the filling capacity of the bladder and causes uncoordinated contractions that can eventually result in enuresis.
Complications of enuresis are primarily psychological, and they include embarrassment, stress, and shame, which can have a strong impact on the client’s self-esteem. Additionally, recurrent loss of urine can cause a skin rash on the genital area or genitourinary infections. The most important clinical manifestation of enuresis is repeatedly urinating in bed or on clothes, resulting in urine-soaked clothes and bed sheets.
Diagnosis of enuresis is based on detailed history and physical assessment, and is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, So, there are four main criteria that must be met in order to confirm the diagnosis of primary enuresis. First, there’s voluntary or involuntary urination into the bed or clothes. Second, this behavior should occur at least 2 times per week for three consecutive months, or cause significant distress. Third, the client must be at least 5 years old; and finally, this behavior should not be associated with some other medication, substance, or medical condition. Moreover, imaging methods, such as ultrasound, an X-ray, and bladder scan can be used to rule out other medical conditions associated with enuresis.