Esophageal atresia and tracheoesophageal fistula: Nursing
Notes
| ESOPHAGEAL ATRESIA AND TRACHEOESOPHAGEAL FISTULA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Esophageal atresia and tracheoesophageal fistula are congenital gastrointestinal anomalies where the esophagus and trachea don’t separate normally during development. Because these two organs develop together and eventually separate, the two conditions often occur together.
Let’s now quickly review the normal development of the esophagus and trachea. They both form from the primitive foregut between weeks 4 and 6 of intrauterine development. Afterwards, they are separated by the tracheoesophageal septum, which divides the foregut into the laryngotracheal tube at the anterior side and the esophagus at the posterior side. Eventually, the laryngotracheal tube develops into the larynx and the trachea, while the esophagus elongates and connects to the stomach.
Now, the exact cause of both esophageal atresia and tracheoesophageal fistula isn’t known, but it has been suggested that environmental factors, along with genetic factors play an important role in their development.
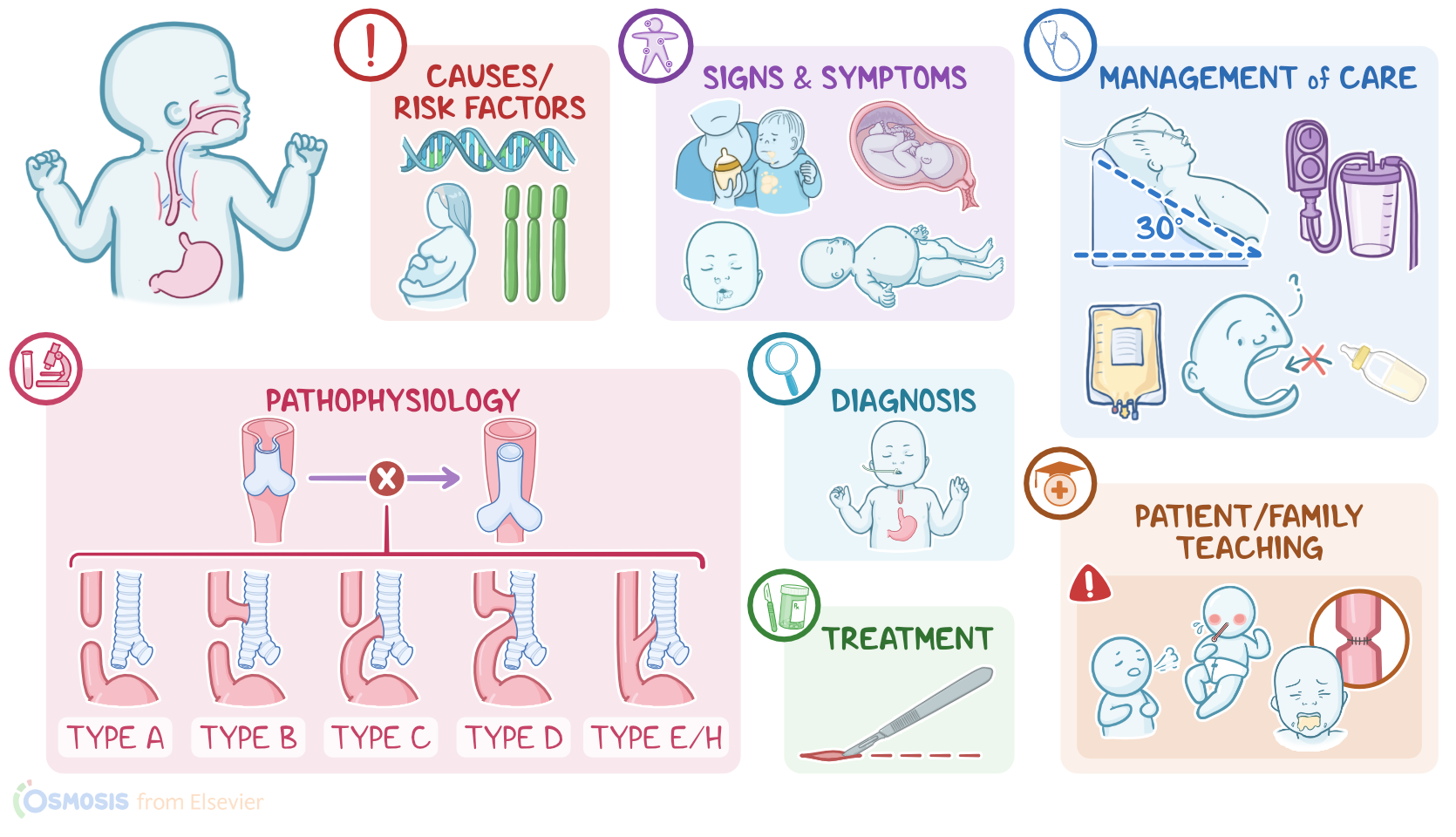
However, there are some risk factors associated with both these conditions. They include prenatal factors, such as maternal use of alcohol and smoking, uncontrolled diabetes mellitus, increased maternal age or exposure to drugs like methimazole and diethylstilbestrol. Risk factors unrelated to maternal ones include chromosomal anomalies, like trisomy 13, 18 or 21 and VACTERL syndrome, which is associated with spinal, anal, heart, tracheoesophageal fistulas, kidneys and limb anomalies.
Now let’s switch gears and look at the pathology of these conditions. With esophageal atresia, the esophagus fails to elongate and connect to the stomach around week 4 of intrauterine development. So essentially, there’s a proximal esophagus that ends in a blind pouch; and a distal esophagus, which ends right above the diaphragm. This is commonly associated with a tracheoesophageal fistula, which is a connection between the trachea and either the proximal, the distal or both parts of the esophagus.
Based on the location and extent of the defect, these two conditions are classified into 5 types. Type A is called isolated esophageal atresia and happens when the middle part of the esophagus is missing. In type B, the proximal esophagus communicates with the trachea. In type C, which is the most common type, there’s proximal esophagus atresia, but this time the distal esophagus has a communication with the trachea. In type D, the middle part of the esophagus is missing, but both the proximal and distal parts of the esophagus communicate with the trachea. Finally, with type E, also referred to as type H, there’s a tracheoesophageal fistula, but no esophageal atresia.
Let’s move on and talk about complications. These include aspiration pneumonia and lung abscesses or bronchiectasis due to recurrent aspiration.
Postoperatively, complications include leaking at the site of anastomosis, strictures, or the formation or return of preexisting tracheoesophageal fistula. Other complications include impaired esophageal motility and resulting gastroesophageal reflux, which increases the risk of recurrent pneumonia and other respiratory problems.
Okay, the most frequent clinical manifestations of esophageal atresia in the prenatal period are polyhydramnios, which happens because the fetus does not swallow amniotic fluid normally; along with the absence of stomach gas on prenatal abdominal echography. Postnatal symptoms and signs include frothy saliva in the mouth and nose and excessive drooling, inability to swallow feedings, vomiting, abdominal distention, and in severe cases, respiratory distress.
Keep in mind the three Cs for esophageal atresia: coughing, choking during feeding, and cyanosis. With tracheoesophageal fistula, when the proximal esophagus is connected to the trachea, the above symptoms remain, but there’s a higher chance of developing aspiration pneumonia when content from the esophagus reaches the lungs. This is associated with respiratory symptoms, like respiratory distress, along with systemic symptoms like malaise and fever. When the distal esophagus is connected to the trachea, GI symptoms like gastric distention appear, due to the fact that air reaches the stomach through the fistula.
Diagnosis of both conditions start with a full history and clinical exam. Clinically, a nasogastric or an orogastric tube wouldn’t be able to pass all the way from the mouth to the stomach. Imaging exams include abdominal X-rays, where you can see a large gastric bubble in types C, D, and E, but not in type A and B, since in these two there isn’t a communication between the distal esophagus and trachea.
Chest X-rays with a water–soluble contrast solution injected through the orogastric tube shows the anomalies and gives the final diagnosis. Additionally, anomalies that include the VACTERL syndrome should be assessed.
Treatment-wise, surgery is the only effective means to correct these conditions; and in otherwise healthy, term newborns, immediate repair is indicated. Other options include delayed repair and staged repair, and these can be considered in infants with low or very low birth weight, moderate or severe pneumonia, or other severe comorbidities or defects.
Sources
- "Foundations of Maternal-Newborn and Women's Health Nursing" Elsevier (2019)
- "Essentials of Pediatric Nursing" LWW (2021)
- "Saunders comprehensive review for the NCLEX-RN examination" Elsevier (2017)
- "Merenstein & Gardner’s handbook of neonatal intensive care: An interprofessional approach" Elsevier (2021)
- " First Aid for the USMLE Step 1 2021" McGraw-Hill Education (2021)
- "Larsen's human embryology" Elsevier (2015)
- "Fetal and Neonatal Physiology (5th ed.)" Elsevier (2017)
- "Tracheoesophageal Fistula" NeoReviews (2021)
- "Esophageal Atresia" Pediatric Surgery Handbook for Residents and Medical Students (2021)