Hirschsprung disease: Nursing
Notes
| HIRSCHSPRUNG DISEASE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Hirschsprung disease is a congenital condition in which neural ganglia or clusters of nerves from segments of the colon are missing, which ultimately leads to a blocked colon, causing it to enlarge. This is why sometimes it’s also referred to as intestinal aganglionosis or just congenital megacolon.
Okay, so the intestines move the waste through the bowels in one direction only, via coordinated wave-like smooth muscle contractions called peristalsis. This is controlled by the autonomic nervous system, which is divided into two parts; the sympathetic, and the parasympathetic nervous systems. The sympathetic nervous system is our fight or flight response and increases heart rate, while slowing down digestion through reducing peristalsis. On the other hand, the parasympathetic nervous system is our rest and digest response and it slows down heart rate, and increases digestion by promoting peristalsis.
Now, if we look closely at the intestinal smooth muscle layer, it’s actually composed of a circular and a longitudinal muscle layer. Within these layers are two plexuses, or networks of nerves made up of ganglia, which are clusters of individual parasympathetic ganglion cells. First there’s the myenteric plexus, also known as Auerbach’s plexus, which when activated, primarily causes smooth muscle relaxation. The myenteric plexus connects with the submucous plexus, or also known as Meissner’s plexus, which is buried in the submucosa and is responsible for helping to control blood flow and epithelial cell absorption and secretion.
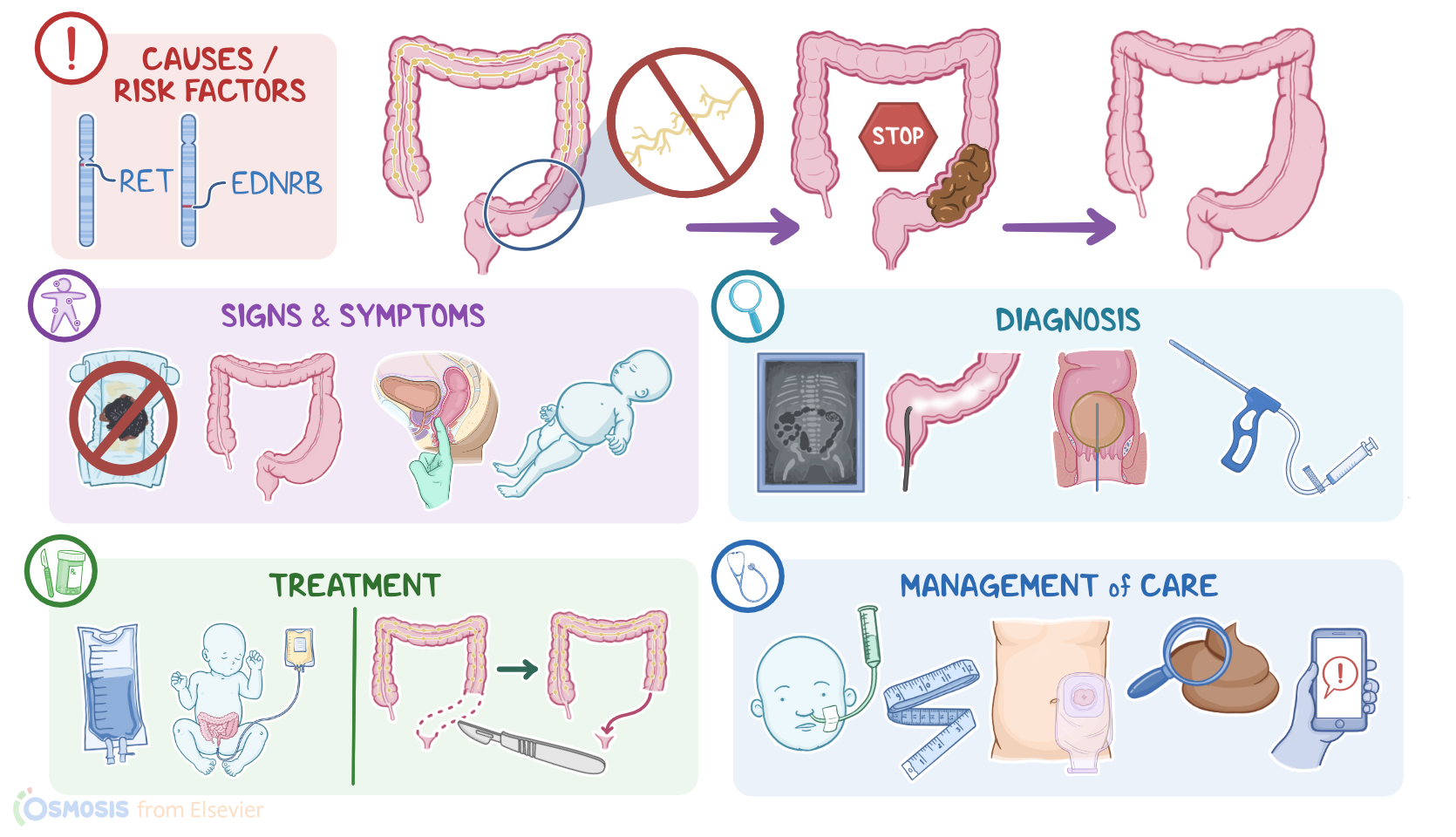
Now, these two nerve plexuses are formed during early stages of fetal development when a group of fetal cells called neural crest cells start differentiating into neuroblasts. Around week 4 of development, these neuroblasts start migrating from the mouth towards the anus. Around week 8, they get to the proximal colon of the gut, and pass through the distal colon, and around week 12 they finally reach the rectum. Two specific genes that are thought to be important for migration and development of these nerve fibers are RET and EDNRB.
Hirschsprung disease can be caused by mutations in either the RET or EDNRB genes. Also, mutations in these genes have been linked to Down syndrome, Multiple Endocrine Neoplasia type 2, or MEN 2, and Waardenburg syndrome, which might help explain why these syndromes are associated with Hirschsprung disease.
So, these genetic mutations can cause disruption of the neuroblast journey towards the anus. As a result, in the rectum and parts of the colon, there’s no development of parasympathetic ganglion cells in the nerve plexuses. The absence of parasympathetic ganglion cells results in unopposed sympathetic stimulation of the intestines, which are unable to relax and remain in a state of sustained contraction. Ultimately, this results in a lack of peristalsis, which essentially blocks the movement of feces.
Clients that are born with Hirschsprung therefore fail to pass the meconium, their first stool, a process that usually happens within the first 2 days after birth. The rectum and the distal sigmoid colon, which are the areas closest to the anus are usually affected, so feces builds up before the obstruction, which causes serious constipation. Hence, a digital rectal examination of the newborn often leads to explosive passage of gas and watery stools known as squirt or blast sign. Excessive constipation can also lead to massive colon dilation, or megacolon, which in turn causes abdominal distention, and increases the risk for rupture of the bowel. infants may also present with bilious vomiting, poor feeding, refusal to feed and failure to gain weight, while older children can present with chronic constipation. . Diagnosis of Hirschsprung disease starts with the client’s history and physical assessment, followed by an abdominal X-ray. This might show an enormous megacolon full of stool with the possibility to localize the affected segment and determine its length. In addition, barium enema or water-soluble contrast enema can be performed to reveal a dilated colon proximal to aganglionic region. Anorectal manometry can be also done to show the lack of relaxation of the internal anal sphincter. Finally, diagnosis can be confirmed by performing a rectal suction biopsy of the narrowed area in the colon which shows the absence of the ganglion cells.
Treatment of Hirschsprung disease includes non-surgical and surgical options. Non-surgical management involves relieving chronic constipation with stool softeners, as well as rectal irrigation with normal saline. Hydration is maintained with IV fluids and electrolytes. In case of abdominal distention, a nasogastric tube is placed. Finally, IV antibiotics are given to limit the risk of infections. The mainstay of treatment, though, is surgical resection of the aganglionic part of the colon, followed by connecting the healthy end to the anus.
All right, let’s look at the nursing care you’ll provide for an infant client with Hirschsprung disease. Your priority nursing goals are to promote adequate bowel elimination, monitor for complications, and provide supportive care, including the psychosocial needs of the child’s parents or caregivers.
While caring for your client postoperatively, be sure to keep them NPO, or nothing by mouth; maintain their nasogastric tube, or NG tube, at low-intermittent suction; administer IV fluids, antibiotics, and pain medications as ordered; and provide emotional support for the child’s caregivers. In addition, closely monitor your client’s vital signs, fluid intake and output, and measure your client’s abdominal circumference. Immediately report if your client presents signs of enterocolitis, including fever, abdominal distension, or explosive, foul-smelling diarrhea.
If a temporary colostomy was performed, assess the site, noting normal findings, such as a pink or rosey red stoma with minimal swelling or bleeding; a stoma that stays well above the level of the skin with colostomy bag securely in place; and intact skin surrounding the stoma. Immediately report to the healthcare provider right away if you notice increased bleeding or swelling; signs of ischemia like a dusky or blue stoma; or if you notice signs of retraction, including a flattening of the stoma or if it starts to move below the level of the skin. On the other hand, if the child does not have a colostomy, monitor their output from the bowel, and provide scrupulous care for the skin around the anus.
When peristalsis returns, discontinue the NG tube and start your client on clear liquids. Closely monitor the color, consistency, and amount of stool. Be sure to report if your client presents signs of an obstruction, including vomiting, abdominal distension, or an absence of gas or stool.