Intrapartum assessment - Uterine activity: Nursing
Notes
| INTRAPARTUM ASSESSMENT - UTERINE ACTIVITY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
Transcript
Content Reviewers
Contributors
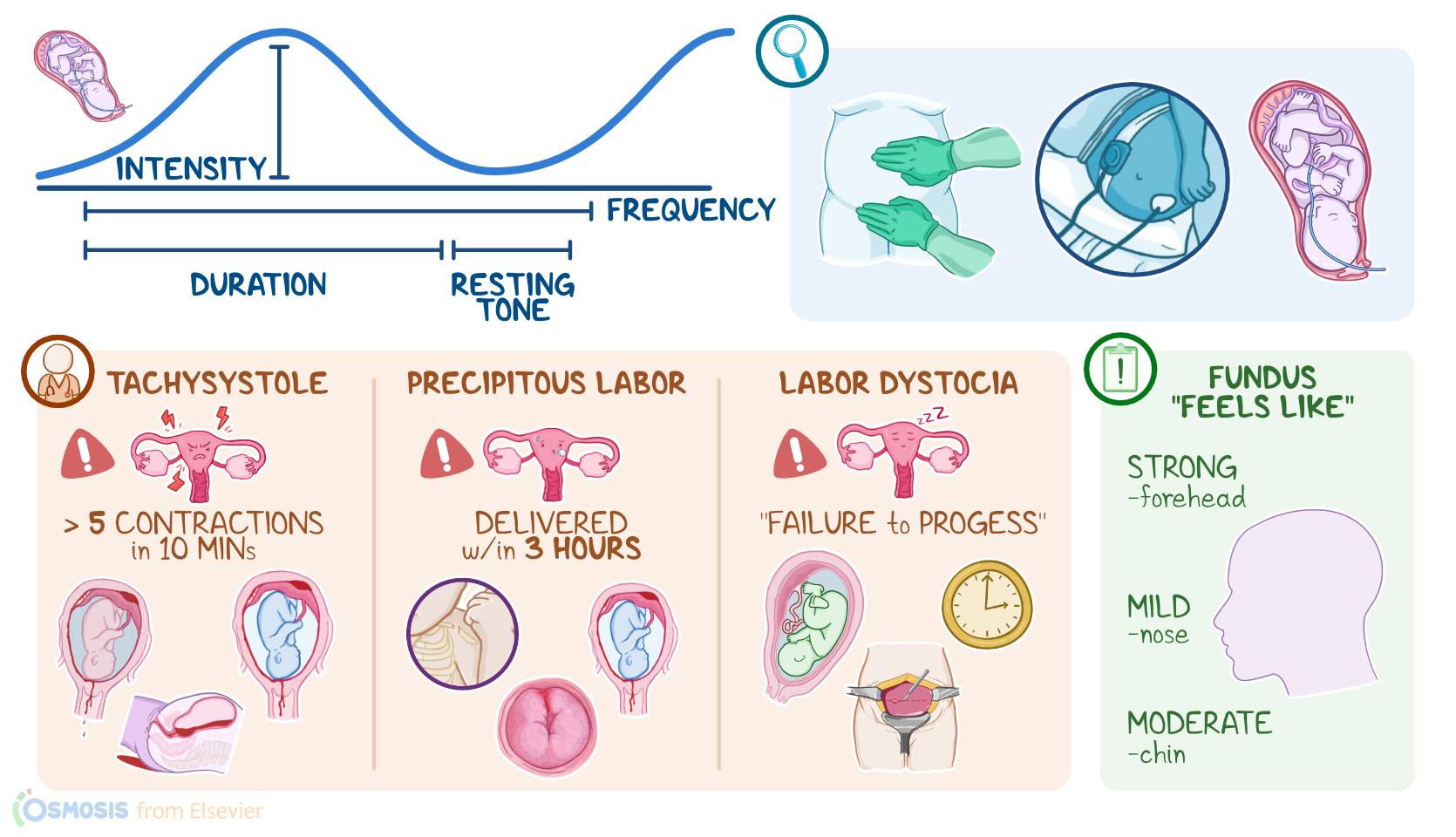
The intrapartum period refers to the time of pregnancy from the onset of labor to delivery of the newborn and the placenta. During this period, the uterus contracts to provide the main force necessary for delivery. So intrapartum assessment of uterine activity refers to assessing the frequency, duration, and intensity of these contractions. Of note, the assessment of the fetus during labor is always interpreted relative to uterine activity.
First, let’s go over the physiology of the uterus, which is a pear-shaped, hollow, muscular organ that protects and nurtures the fetus, but also promotes its delivery during labor. The superior part of the uterus is called the fundus, the middle part is the body and the bottom, cylindrical portion is the cervix. Zooming in, the uterus has three layers: the outer serosal layer, or perimetrium; the middle muscular layer, or myometrium; and the inner mucosal layer, or endometrium.
The myometrium consists of smooth muscle fibers, which can tighten to produce uterine contractions in response to certain hormones, like oxytocin. Now, the number of oxytocin receptors in the myometrium are low during most of the pregnancy, but they increase dramatically during the third trimester, reaching the greatest concentration during active labor. The oxytocin receptors, especially those in the fundus, respond to oxytocin by promoting rhythmic synchronized endometrial contractions from the fundus towards the cervix, causing dilation and effacement, or thinning of the cervix, as well as pushing the fetus through the birth canal. Normal uterine activity during labor involves 5 contractions or fewer in a 10 minute period, averaged over 30 minutes. Between contractions, the uterus relaxes to allow adequate blood flow to the placenta and fetus.
Now, let’s switch gears and go through some types of dysfunctional labor. First up, is tachysystole, which is defined as more than 5 contractions in a 10 minute period, averaged over 30 minutes.This is caused by the uterine muscle’s inability to properly relax between contractions, compromising blood flow to the uterus, placenta and fetus. The most common cause of tachysystole is excessive administration of exogenous oxytocin or prostaglandins. This can cause problems like placental abruption, which is when the placenta separated prematurely from the uterine wall; as well as postpartum hemorrhage. The fetus can also experience hypoxia due to the rapid contractions.
Another type of dysfunctional labor is precipitous labor, or rapid labor, where the fetus is delivered within 3 hours from the onset of labor. These frequent contractions can cause maternal injuries such as lacerations of the cervix, vagina, and outer genitalia; as well as placental abruption; and postpartum hemorrhage. The fetus can also experience hypoxia due to the rapid contractions, or even injuries.
On the other hand, labor dystocia, or slow, abnormal contractions, is ineffective in progressing cervical dilation and effacement, and fetal descent. This type of dysfunctional labor is sometimes referred to as “failure to progress.” These contractions are infrequent, weak, and brief, and can slow the progression of labor; cause complete arrest of labor; result in the exhaustion of the client; as well as increasing risk for infections and neonatal sepsis. Clients experiencing labor dystocia will often require cesarean birth.