Multiple gestation: Nursing
Multiple gestation: Nursing
Gyno, prenatal, pregnanct care
Gyno, prenatal, pregnanct care
Notes
| MULTIPLE GESTATION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
Transcript
Multiple gestation or multifetal pregnancy describes pregnancy with more than one fetus at a time. The most common type of multiple gestation is twin pregnancy, meaning a pregnancy with two fetuses.
All right, now let’s quickly review the physiology of fertilization, starting with the ovaries, which are the paired female gonads. Each month, they release one mature egg, also called oocyte, which is the female gamete. After leaving the ovaries, the egg enters the fallopian tube and reaches the widest part of it, called the ampulla of the fallopian tube. This is where the few sperm that have made it this far after ejaculation surround the egg; and of them, a single sperm succeeds in entering the egg and fertilizing it, forming the zygote.
The zygote then makes its way through the fallopian tube in order to reach the uterus; and at the same time, it undergoes mitosis, meaning it divides over and over again into smaller cells called blastomeres. When there are 32 blastomeres, the fetus is called a morula. At about day four after fertilization, a fluid cavity appears inside the morula to form the blastocyst, which contains an inner and outer group of cells. About six or seven days after fertilization, the blastocyst reaches the uterus and implants in the inner lining of the uterus, called the endometrium.
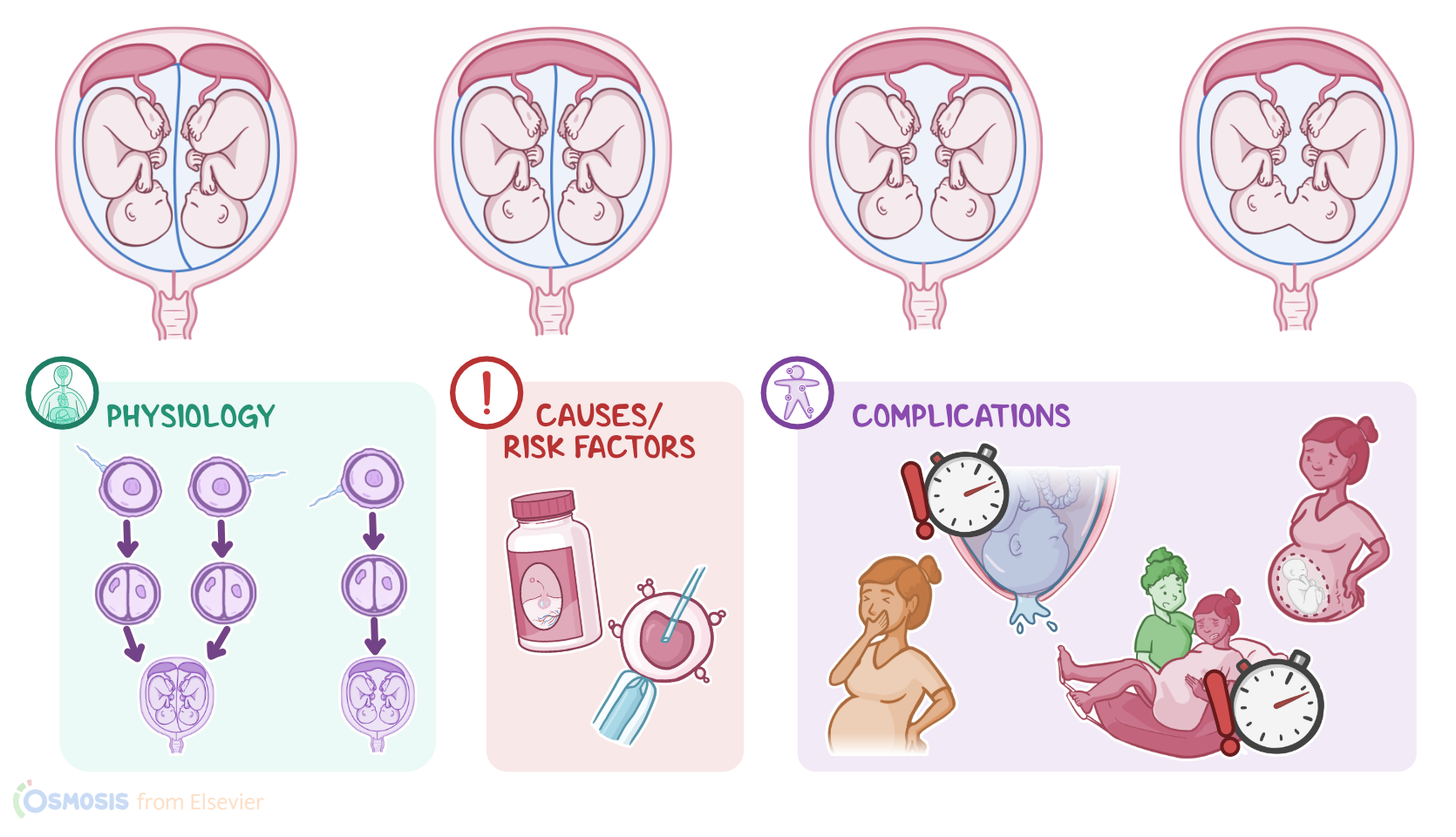
Now, multiple gestation typically happens when the ovaries release more than one oocyte in a particular month, and more than one sperm ends up fertilizing them; one for each. This gives rise to dizygotic twins, also called fraternal or non-identical twins; because the two zygotes develop individually. Alternatively, multiple gestation can occur when the zygote divides into two separate zygotes shortly after fertilization. This situation gives rise to monozygotic, also called identical twins.
Now, multiple gestation differs between monozygotic and dizygotic twins. With monozygotic twins, if the division of the zygote in two happens at the morula stage, that means each of the twins will have their own placenta and their own amniotic sac; so they are called dichorionic, diamniotic twins. Alternatively, if the division happens at the blastocyst stage, there will be only one placenta and two amniotic sacs, so they’re called monochorionic diamniotic twins. Additionally, if the division happens after implantation, there will be one placenta and one sac for both twins; so they’re called monochorionic monoamniotic twins. Finally, if the division happens long after implantation, the twins will be physically connected to each other, called conjoined twins.
On the other hand, dizygotic twins implant at different sites in the endometrium and develop separately, each with their own placenta and amniotic sac. The chances of a multiple gestation occuring are increased when using ovulation stimulation medications, such as clomiphene citrate and follicle stimulating hormone, as well as using assisted reproductive technologies, also known as in-vitro fertilization or IVF for short. The chances of multiple gestation also increases if there’s a personal or family history of multiple gestations, advanced maternal age, Black race, in addition to high parity, meaning having had five or more pregnancies in the past.
Multiple gestation can increase the risk of certain complications, these can be grouped into complications during pregnancy, complications related to delivery, and complications after delivery. Complications during pregnancy include spontaneous abortion; premature rupture of membranes; preterm labor; anemia; hyperemesis gravidarum, meaning excessive nausea and vomiting; gestational hypertension and preeclampsia; intrauterine growth restriction; congenital anomalies; twin to twin transfusion syndrome, when there is a shared placenta, and one twin gives away more blood than it receives leading to malnourishment and oligohydramnios, which is a reduction in amniotic fluid, while the other twin receives too much blood, develops polyhydramnios or too much amniotic fluid, and can develop cardiac problems; as well as vanishing twin syndrome where there’s loss of one of the embryos.