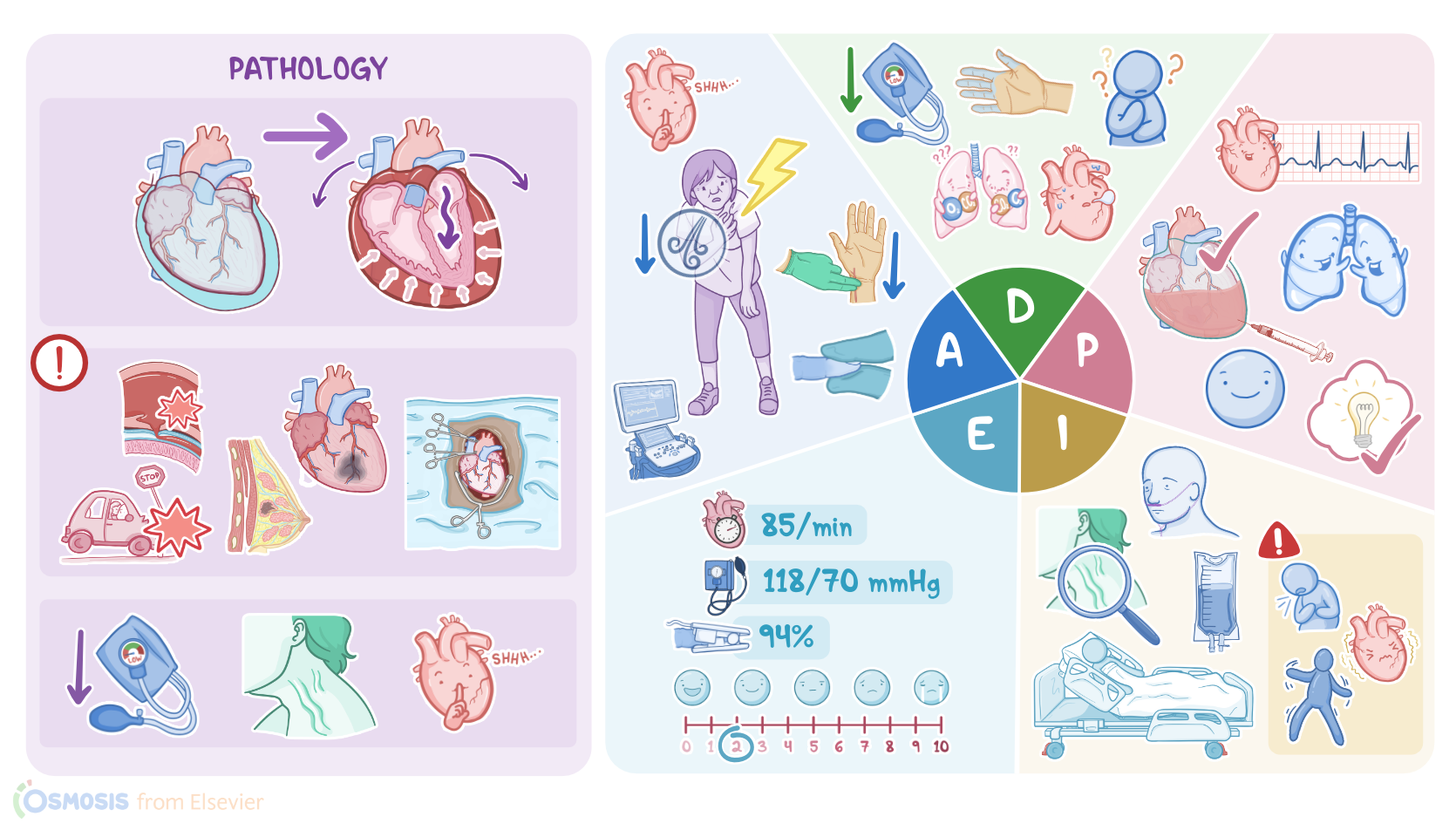
Pericardial effusion and cardiac tamponade: Nursing process (ADPIE)
Notes
| PERICARDIAL EFFUSION AND CARDIAC TAMPONADE | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Lydia Smith is a 42-year-old female client with a history of metastatic breast cancer currently being treated with radiation therapy.
She presents with shortness of breath and chest pain while at the radiation therapy clinic this morning.
She states she started having intermittent chest pain two days prior that feels like heavy pressure under her sternum.
Her radiation treatment is postponed temporarily, and her oncologist sends her for several cardiac tests including a chest x-ray, electrocardiogram or ECG, and an echocardiogram, to determine the cause of her symptoms.
Her cardiac test results confirm a large pericardial effusion, and she is directly admitted by her oncologist to a telemetry unit pending pericardiocentesis.
When extra fluid builds up in the pericardial cavity, it is known as pericardial effusion, which can then develop into cardiac tamponade depending on how much extra fluid there is and how quickly it accumulates.
Cardiac tamponade puts pressure on the outside of the heart restricting its movement.
As a result, the heart is unable to pump normally, causing compromised cardiac functioning and resulting in decreased cardiac output.
The heart sits inside a two-layered pouch called the pericardium.
Within this pouch there is the pericardial cavity which is filled with a small amount of fluid that lets the heart slip around as it beats.
Typically, there is approximately 15 to 50 milliliters of fluid in the pericardial cavity at any given time.
The pericardial cavity can stretch to accommodate a gradual accumulation of fluid without immediate adverse effects.
When fluid accumulates gradually, the pericardium can hold as much as 1.5 liters of fluid before tamponade sets in.
In contrast, if there is a rapid buildup of fluid, even as little as 100 milliliters, does not allow the pericardial cavity to stretch and can compress the heart, leading to cardiac tamponade.
A rapid accumulation of fluid can occur as a result of trauma to the chest.
For example, a stab wound can puncture a blood vessel and fill the pericardium with blood, or blunt trauma like hitting your chest with a steering wheel during a car crash causing the rupture of many small blood vessels.
Another cause is aortic dissection, which is when an injury to the innermost layer of the aorta allows blood to flow between the layers of the aortic wall, forcing the layers apart.
If the aortic dissection ruptures through the wall of the aorta and through the fibrous pericardium, blood can spill right into the pericardial cavity, leading to cardiac tamponade.
Cardiac tamponade can also occur a few days after a myocardial infarction or heart attack, because the weak ventricular wall can rupture when exposed to the high ventricular pressure.
A rare cause is heart surgery, where, once again, a weakened muscle can rupture and cause cardiac tamponade days after the operation.
The improper insertion of a central line or pacemaker can also increase the risk for cardiac tamponade due to the heart being perforated during the insertion or catheter migration post insertion.
Other causes of cardiac tamponade involve long-term factors.
In these cases, the fluid accumulates from a chronically inflamed pericardium that can’t resorb pericardial fluid as quickly as it builds up.
Examples of this include cancers that have spread to the pericardium, such as breast or lung cancer, certain cancer treatments such as radiation therapy to the chest wall, or pericarditis which is the inflammation of the pericardium from infection.
Cardiac tamponade has a classic clinical presentation which includes a combination of symptoms known as Beck’s triad.
This includes hypotension, distended neck veins, and distant or muffled heart sounds.
If cardiac tamponade develops, fluid puts pressure on the heart and prevents it from fully stretching or relaxing between contractions.
As a result, the cardiac chambers can’t fill with blood properly which causes a decrease in cardiac output leading to hypotension.
The accumulation of fluid also makes it difficult for the atria to expand enough to accommodate venous blood returning to the heart.
As a result, the blood will have nowhere to go but back into the veins.
This is why you may see distended jugular veins when you look at the neck of a person with cardiac tamponade.
When listening to the chest, fluid accumulation can result in muffled or distant heart sounds.
Other symptoms that can be present includes pulsus paradoxus, which is when the systolic blood pressure drops more than 10mmHg during inspiration.
Tachycardia results because less blood leaving the heart means less blood is reaching the organs and tissues, so the heart tries to compensate for the low output by beating faster.
This decreased cardiac output can also lead to weak peripheral pulses.
Pressure from the fluid accumulation can also cause chest pain or discomfort.
Decreased cardiac output can cause dyspnea because there is less blood flow to the lungs.
As cardiac tamponade progresses, the heart can ultimately become ischemic and stop beating altogether.
This dangerous situation requires immediate intervention.
A diagnosis of cardiac tamponade often starts with an electrocardiogram or ECG.
Classic findings include sinus tachycardia, a low QRS complex voltage, and electrical alternans, which is when the QRS complexes have different heights.
However, the most precise diagnostic tool is an echocardiogram, which can show the excess pericardial fluid, and the heart “swinging” around inside the pericardial cavity.
A chest X-ray will show an enlarged pericardial silhouette if the accumulation of fluid is more than 200 millilitres.
Several lab tests including complete blood count, chemistry panel, and cardiac biomarkers can be helpful in determining any contributing factors such as infection.
Cardiac tamponade is treated by inserting a needle directly into the pericardium and draining the pericardial fluid to relieve the pressure surrounding the heart, a process called pericardiocentesis.
The removal of excess fluid with a pericardiocentesis results in dramatic improvement in hemodynamic status.
Prior to the procedure, the patient is provided with oxygen therapy and bed rest with the head of the bed elevated to reduce the heart’s workload, IV fluids for volume expansion to increase blood flow, and medication for chest pain. Intake and output should be monitored, in particular urine output since a drop in urine output may indicate decreased renal perfusion.
Following the pericardiocentesis, the underlying disease is addressed.
Now that we understand pericardial effusion and cardiac tamponade, let’s get back to our client Lydia who has now been admitted to a telemetry unit.
Her pericardiocentesis has been scheduled for the following day.
After entering her room, you introduce yourself, wash your hands, and confirm her identity.
You ask her how she is doing, and she says she is anxious about her procedure tomorrow.
She also states she has been having chest pain and shortness of breath the last few days.
She rates her chest pain as a 6 out of 10 on a 0-to-10 scale.
Key Takeaways
Pericardial effusion is a condition in which there is an abnormal accumulation of fluid in the pericardial sac. This can happen due to a variety of causes, such as infections, autoimmune diseases, cancer, heart attack, and radiation therapy. Symptoms of pericardial effusion include chest pain, shortness of breath, and difficulty breathing when lying down.
Cardiac tamponade is a serious complication of pericardial effusion, in which the accumulated fluid puts pressure on the heart and prevents it from working properly. Cardiac tamponade is characterized by the classic Beck's triad, which is hypotension due to impaired cardiac output, jugular venous distention due to blood backing up, and muffled heart sounds on auscultation. The treatment of both conditions involves pericardiocentesis and addressing the underlying condition.
Sources
- "Management of Acute and Recurrent Pericarditis: JACC State-of-the-Art Review" J Am Coll Cardiol (2020)
- "Cardiac tamponade secondary to Dressler's syndrome" BMJ Case Rep (2021)
- "Pericardial Effusion Provoking Atrial Fibrillation After Cardiac Surgery: JACC Review Topic of the Week" J Am Coll Cardiol (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "New Approaches to Management of Pericardial Effusions" Curr Cardiol Rep (2021)
- "Pericardial effusion" J Bras Pneumol (2021)
- "Pericardial effusion and tamponade in a young woman" Ann Acad Med Singap (2022)