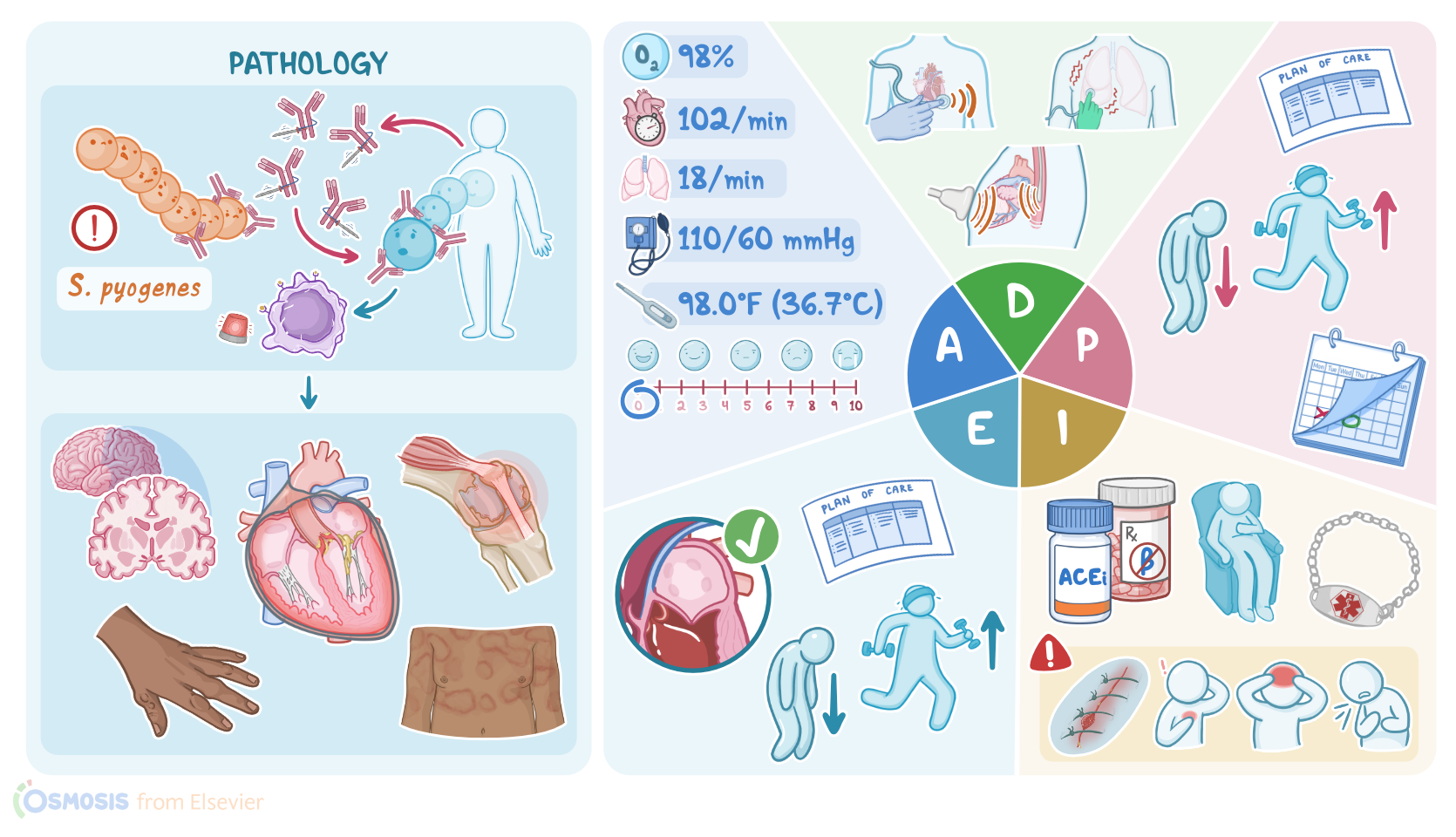
Rheumatic heart disease: Nursing process (ADPIE)
Rheumatic heart disease: Nursing process (ADPIE)
gap test med surg
gap test med surg
Notes
| RHEUMATIC HEART DISEASE (RHD) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Saanvi Kumar is a 17-year-old female client who recently immigrated from India. Saanvi has a history of recurrent rheumatic fever with the last episode resolving 10 years ago. Lately, Saanvi noticed she feels more tired than usual and started feeling short of breath during gym class, so her pediatrician referred her to a cardiologist for further evaluation. The cardiologist ordered an echocardiogram, a chest X-ray, and an electrocardiogram, or ECG, and Saanvi is diagnosed with rheumatic heart disease.
Rheumatic heart disease is a complication of rheumatic fever, which is a delayed multisystemic inflammatory condition that typically occurs two to four weeks after a strep throat infection. Strep throat is caused by bacteria called Streptococcus pyogenes, which is often referred to as group A beta hemolytic streptococcus or GAS for short. Not everyone who has strep throat will develop rheumatic fever, but it’s important to note that children between the age 5 and 15 are at a higher risk.
Rheumatic fever arises because Streptococcus pyogenes has a bacterial protein that mimics the structure of some proteins in the human body. So, when the immune system produces antibodies against the bacterial protein, these antibodies also end up targeting our own tissue. The heart is one of the major organs affected but others include the joints, skin, and brain. Once bound to human proteins, these antibodies activate nearby immune cells, which induce an inflammatory response that leads to tissue destruction and fever.
Now let’s focus on the inflammation of the heart, which is also known as carditis. Clients with rheumatic fever typically develop pancarditis, which is the inflammation of all three layers of the heart: endocardium, myocardium, and pericardium. But, if a client repeatedly experiences attacks of rheumatic fever, chronic inflammation of the heart can lead to leaflet damage and valvular lesions. This condition is called rheumatic heart disease and it's most commonly associated with valvular heart disease called mitral regurgitation. In mitral regurgitation, valve leaflets do not form a tight seal and this results in an abnormal blood flow from the left ventricle back into the left atrium during systole. This can result in left-sided heart failure where the left side of the heart can’t pump blood effectively, causing blood to back up into the lungs and pulmonary edema.
Next, there are some extracardiac manifestations, which include a ring shaped rash on the skin, typically on the arms or trunk called erythema marginatum. There can be painful subcutaneous nodules which are firm lumps usually found over bony prominences. Multiple large joints can also become inflamed leading to transient arthritis. Finally, in the central nervous system, the basal ganglia can be affected leading to chorea which involves involuntary jerky movements of the arms leg and face.
These five signs constitute the major diagnostic criteria for rheumatic fever, which are known as the Jones criteria. But, there are also some minor criteria that help make the diagnosis, such as fever, joint pain, changes in a client’s electrocardiogram, and elevated acute-phase reactants, which are proteins that increase in the blood in response to inflammation.
Now, in contrast to rheumatic fever, the diagnosis of rheumatic heart disease starts with a physical exam. Typical auscultation finding in clients with mitral regurgitation is a holosystolic murmur, also known as a pansystolic murmur. This means that murmur lasts for the duration of systole and that’s because the blood is flowing back into the left atrium. The sound is a high-pitched, blowing murmur that is loudest at the apex of the heart and radiates toward the axilla. If heart failure has developed, the client’s peripheral pulses may be weak and thready, and their extremities may be cool and clammy. The client may experience dyspnea and lung sounds may reveal crackles.
Imaging methods are also used to identify mitral regurgitation and the diagnostic method of choice is echocardiography, which can be transthoracic or transesophageal. Transthoracic echocardiography or TTE, is a non-invasive method performed over the client’s chest wall; while transesophageal echocardiography or TEE, is an invasive method that requires the insertion of a flexible transducer into their esophagus. Other diagnostic methods, such as chest X-ray and ECG, cannot detect valvular lesions but only heart abnormalities, such as enlargement of the left atrium. Finally, the treatment of clients with mitral regurgitation requires valve repair or surgical replacement of the valve.
All right, it’s time to begin Saanvi’s assessment. After introducing yourself to Saanvi and Mr. Kumar, performing hand hygiene, and confirming her identity, you ask Saanvi how she has been feeling. She says she’s been tired, especially for the past few months. She adds, “I’m having a hard time keeping up in gym class. Sometimes I feel like I can’t catch my breath and my heart is pounding like crazy.” Mr. Kumar mentions that most days Saanvi needs to take a nap after school, which is unlike her because she would much rather hang out with friends. You note Saanvi is sitting comfortably on the exam table and does not appear to be in distress. As you begin her physical assessment, you note she has 2+ pitting edema in both feet. Her skin is warm, intact with good turgor and no rashes are present. She denies having a sore throat, and her throat appears pink, moist, and without lesions. Her jugular veins are nondistended and lymph nodes are not swollen.