Urticaria: Nursing
Urticaria: Nursing
Patho Final
Patho Final
Notes
| URTICARIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Contributors
Urticaria, also commonly known as hives, is a skin reaction characterized by wheals, which are raised, pruritic areas that are erythematous or red with central pallor and clearly defined borders.
Now, let’s quickly review the physiology of skin reactions. The skin is the outer barrier that protects the body from any external threat like pathogens or antigens. To do this, the skin has a thick outer layer called epidermis, which in turn consists of multiple cell layers. Below the epidermis, there’s a deeper layer called the dermis, which is mostly made of connective tissue, and contains structures like hair follicles, nerve endings, and blood vessels. Within the dermis, there’s also a special type of immune cell called mast cells, which serve as a first line of defense to trigger an immune response when they sense an external threat.
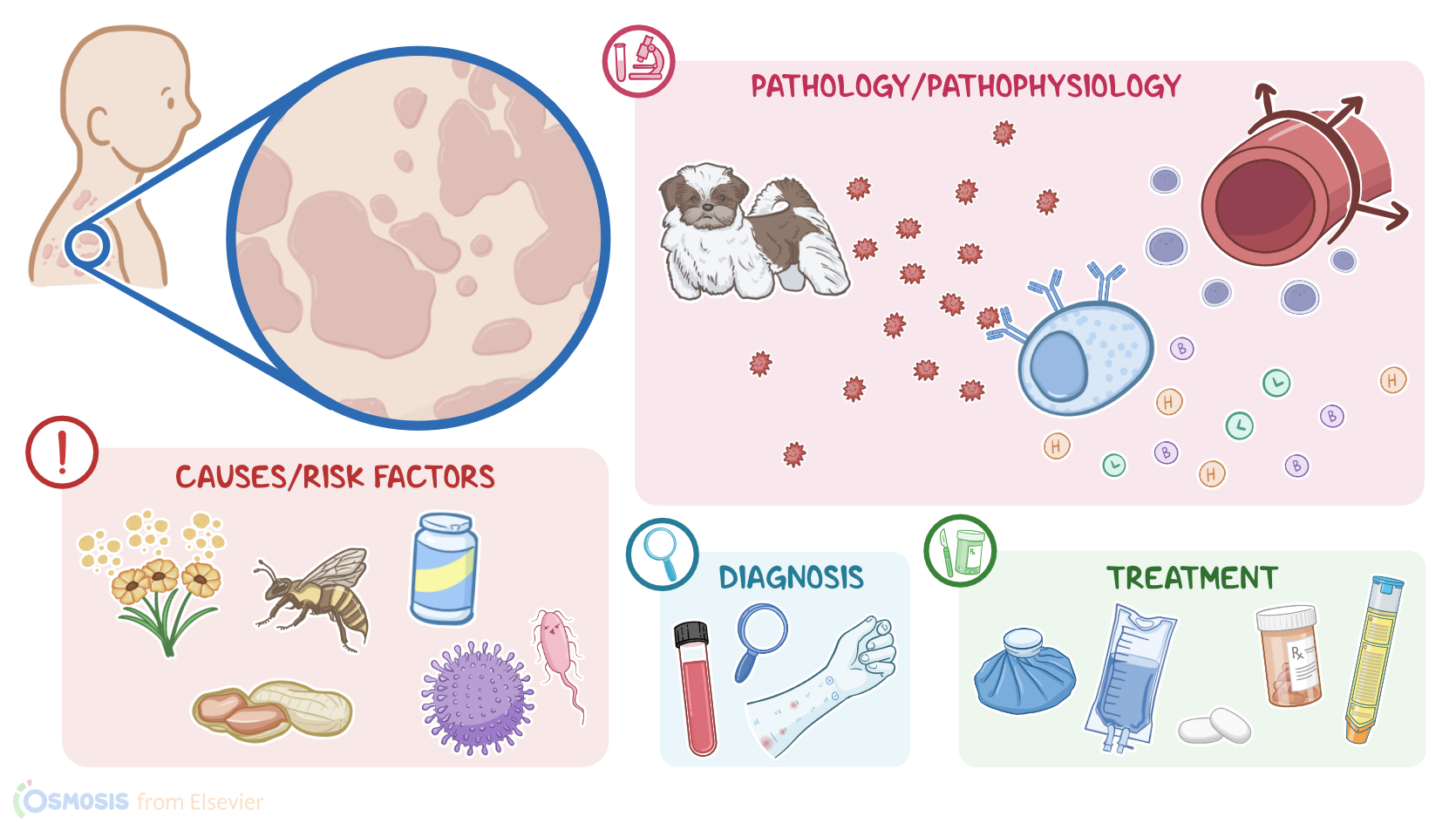
Now, urticaria is typically caused by exposure to allergens, such as pollen, pet dander, dust, bee stings, latex, and food like shellfish and nuts, as well as certain medications like antibiotics or NSAIDs. Other common causes include viral, bacterial, or parasitic infections.
Less frequently, urticaria can be caused by stress, exercise, sweat, exposure to extreme temperatures or sunlight, as well as vibration, friction, or pressure against the skin. Finally, urticaria can also be idiopathic, meaning that the cause is unknown.
Risk factors for developing urticaria include having allergies or a family history of allergies or urticaria; as well as frequent infections, stress, cold or heat exposure, taking certain medications, and having an autoimmune disease like lupus.
Okay, the underlying pathology of urticaria is a type I hypersensitivity reaction. So, the first time a client is exposed to an allergen, the immune system reacts by producing allergen-specific IgE antibodies, which in turn bind to the surface of mast cells in the skin and mucosa. If the client is exposed to that same antigen again, the IgEs allow mast cells to quickly recognize that antigen. As a result, mast cells become activated and release a large amount of inflammatory mediators, such as histamine, leukotrienes and bradykinin, causing the nearby blood vessels to dilate and increase their permeability, which allows leakage of fluid and attracts more immune cells locally.
Typically, the clinical manifestations of urticaria begin within two to three hours after allergen exposure. Clients generally develop slightly raised, well-defined wheals that are usually red, and blanch with pressure. In addition, these wheals are often very itchy and warm to the touch. Occasionally, urticaria can be accompanied by angioedema, which is characterized by local vasodilation at the subcutaneous and submucosal tissue, leading to increased vascular permeability and tissue swelling; this is most common on the face, like around the eyes, but can also involve the lips, tongue, which can progress down to the throat, closing off the airway. In severe cases, urticaria or angioedema can worsen and cause anaphylaxis.
Key Takeaways
Urticaria, commonly referred to as hives, is a kind of skin rash notable for pale red, raised, itchy bumps, which can cause a burning or stinging sensation. Lesions are frequently caused by allergic reactions; however, there are many nonallergic causes, such as autoimmune disorders like thyroid disease. Most cases of hives lasting less than six weeks (acute urticaria) are the result of an allergic trigger. Chronic urticaria (hives lasting longer than six weeks) is rarely due to an allergy.
Treatment for urticaria typically involves identifying and avoiding triggers, as well as taking medication to relieve symptoms. Antihistamines are often prescribed to block the release of histamine and reduce itching and swelling. In severe cases, oral or injectable corticosteroids may be prescribed. Nursing management and care focuses on helping to eliminate or reduce the triggering factors, manage symptoms, and monitor for complications. Client and family education focuses on prevention and symptom management.
Sources
- "Lewis’s medical-surgical nursing: Assessment and management of clinical problems (11th ed.)" Elsevier (2020)
- "Medical-surgical nursing: Concepts for interprofessional collaborative care (10th ed.)" Elsevier (2021)
- "Habif’s Clinical Dermatology (7th ed.)" Elsevier (2021)