Phosphodiesterase Inhibitors · What Are They, How Do They Work, What Are They Used For, and More
Published: Mar 04, 2025
Author: Ashley Mauldin, MSN, APRN, FNP-BC•
Editor: Antonella Melani, MD•
Editor: Nimmit Vyas, PharmD
Illustrator: Jillian Dunbar
7-day free trial
Go deeper with Osmosis
Osmosis is a learning platform with videos, questions, and AI tools to help you master topics like this.
Watch quick, visual videos
Practice with Qbank-style questions
Use AI to explain, quiz, and review
Study anytime with the mobile app
No credit card · Cancel anytime
What is a phosphodiesterase inhibitor?
Phosphodiesterase inhibitors are a class of medications that promote blood vessel dilation (vasodilation) and smooth muscle relaxation in certain parts of the body, such as the heart, lungs, and genitals. Phosphodiesterases are a diverse family of enzymes that play a key role in regulating cell functions by indirectly increasing the intracellular levels of cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP), both of which are “second messengers” that regulate the primary effects of hormones and neurotransmitters.
Learn deeper with Osmosis
Master this topic faster with videos, questions, and AI.
Used by 8M+ healthcare learners.
Start free trial
No credit card · Cancel anytime
How do phosphodiesterase inhibitors work?
Phosphodiesterase inhibitors work by inhibiting the phosphodiesterase enzymes, thus preventing them from breaking down cAMP and cGMP molecules in the cell. The production of cAMP and cGMP are regulated by a molecule called nitric oxide, and their function is to help regulate physiological processes by decreasing the levels of calcium in the cell. Ultimately, cAMP and cGMP are broken down by phosphodiesterase enzymes.
What happens when phosphodiesterase is inhibited?
When phosphodiesterase is inhibited, it is not able to break down the cAMP and cGMP. Thus, their levels inside the cell increase, which in turn leads to a decrease in the levels of calcium in the cell. Ultimately, this leads to vasodilation and smooth muscle relaxation in their target tissues.
What are phosphodiesterase inhibitors used for?
Phosphodiesterase inhibitors are classified based on which specific phosphodiesterase enzyme they target. There are 11 families of phosphodiesterase enzymes and PDE inhibitors for each. Among these, the most widely used are four types of phosphodiesterase inhibitors: phosphodiesterase type 5 inhibitors (PDE5 inhibitor), phosphodiesterase type 4 inhibitors (PDE4 inhibitor), phosphodiesterase type 3 inhibitors (PDE3 inhibitor), and nonspecific inhibitors.
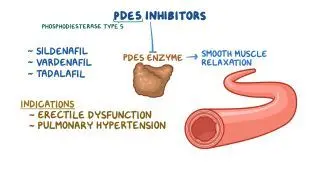
PDE5 inhibitors
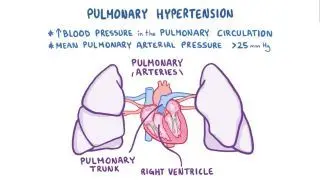
PDE5 inhibitors work by increasing the levels of cGMP and specifically target the penis and the lungs. PDE5 inhibitors can be used to treat erectile dysfunction by inducing smooth muscle relaxation and increasing the blood flow to the penis, leading to an erection. Additionally, PDE5 inhibitors trigger pulmonary vasodilation, helping to regulate the pulmonary perfusion and pressure, thus they can be used to treat pulmonary hypertension when given at a lower dose compared to erectile dysfunction.
PDE4 inhibitorsPDE4 inhibitors work by increasing the levels of cAMP. They specifically target the airways, the skin and immune system, and the brain. PDE4 inhibitors work by causing smooth muscle relaxation in the airways, making them useful in the treatment of pulmonary diseases, such as asthma and chronic obstructive pulmonary disease. PDE4 inhibitors can also be used to treat inflammatory conditions that may affect the skin or other tissues, such as psoriasis, atopic dermatitis, inflammatory bowel disease, and rheumatoid arthritis. There is currently research being conducted on PDE4 inhibitors being used in the treatment of mental conditions, such as depression and anxiety.
PDE3 inhibitors
PDE3 inhibitors work by increasing the levels of cAMP. PDE3 inhibitors are typically used for cardiovascular diseases. In the heart, they help to increase cardiac contractility, or the ability of the heart to beat. They also relax vascular and airway smooth muscle, making them useful in the treatment of heart failure. In addition, PDE3 inhibitors can prevent platelet aggregation into clots, and can thus be used to prevent and treat myocardial infarction (heart attack). Finally, PDE3 inhibitors can trigger vasodilation of peripheral blood vessels and can be used to treat intermittent claudication, which is a cramping in the legs due to a decreased blood flow.
Nonspecific inhibitorsNonspecific inhibitors work by decreasing the destruction of the cAMP by any phosphodiesterase enzyme. They mainly induce mild dilation of the bronchioles of the lungs and help reduce airway inflammation. Nonspecific phosphodiesterase inhibitors are used in the treatment of chronic obstructive pulmonary disease, as well as for short term and long term management of asthma.
What are some examples of common phosphodiesterase inhibitors?
PDE5 inhibitors are the most common and include sildenafil, tadalafil, vardenafil, and avanafil.
The most common PDE4 inhibitors are roflumilast, apremilast, and ibudilast.
Some examples of PDE3 inhibitors are cilostazol and milrinone.
Nonspecific phosphodiesterase inhibitors include theophylline, aminophylline, and methylxanthine.
Is Viagra a phosphodiesterase inhibitor?
Viagra is a PDE5 inhibitor most often used for the treatment of erectile dysfunction. Viagra has also been useful in the treatment of pulmonary hypertension for both short term and long term use when given at a lower dose compared to the dosages prescribed for erectile dysfunction. Viagra has a low number of side effects and is considered relatively safe for individuals with heart disease. However, it’s important to note that the use of Viagra taken along with nitrates can lead to a reduction in blood pressure and is contraindicated.
Are phosphodiesterase 5 inhibitors a competitive inhibitor?
Phosphodiesterase type 5 inhibitors are competitive and reversible inhibitors. When a PDE5 inhibitor is used, it competitively binds to PDE5 to stop it from breaking down cGMP. PDE5 inhibitors are considered reversible because they bind to PDE5 for a limited amount of time. With the decrease in the levels of the cGMP, this will reverse the smooth muscle relaxation in the penis, which will end the erection.
Is caffeine a phosphodiesterase inhibitor?
Caffeine is a phosphodiesterase inhibitor that has been shown to increase the levels of cAMP in the cell thus leading to smooth muscle relaxation. Caffeine is a weak inhibitor, but variations of caffeine including theophylline have been introduced as treatments for pulmonary disease.
Are methylxanthines phosphodiesterase inhibitors?
Methylxanthines are among the first phosphodiesterase inhibitors to be discovered, and are nonspecific. The most common methylxanthine is theophylline, which is commonly used for short or long term treatment of different types of pulmonary diseases, such as asthma. Methylxanthines can help to induce bronchodilation and reduce airway inflammation.
What are the side effects of phosphodiesterase inhibitors?
Common side effects of PDE5 inhibitors include headache, nasal congestion, dyspepsia and flushing. A potential rare side effect of PDE5 inhibitors is priapism, or an erection lasting longer than 4 hours. Priapism is a medical emergency that requires immediate intervention. First line treatment is oral terbutaline or pseudoephedrine. If the priapism persists, needle aspiration of the blood in the penis, as well as an intracavernous injection of phenylephrine, may be needed.
Potential side effects of PDE4 inhibitors are headaches, nausea, and diarrhea.
The most common side effects of PDE3 inhibitors include ventricular arrhythmias, headaches, and hypotension.
Side effects of nonspecific inhibitors include upset stomach, diarrhea, headaches, and restlessness.
What are the most important facts to know about phosphodiesterase inhibitors?
Phosphodiesterase inhibitors prevent the phosphodiesterase enzymes from breaking down cAMP and cGMP in the cell. As a result, they increase the cAMP and cGMP, leading to an increase in intracellular calcium, which causes vasodilation and smooth muscle relaxation. There are four types of phosphodiesterase inhibitors, which have an effect on different locations in the body, depending on the specific phosphodiesterase enzyme they target. PDE5 inhibitors are commonly used for the treatment of erectile dysfunction and pulmonary hypertension. PDE4 inhibitors can be used to treat asthma, chronic obstructive pulmonary disease, psoriasis, atopic dermatitis, inflammatory bowel disease, and rheumatoid arthritis. PDE3 inhibitors are indicated for the treatment of heart failure, coronary heart disease, and to prevent myocardial infarction. Finally, nonspecific phosphodiesterase inhibitors are used in the treatment of asthma and chronic obstructive pulmonary disease.

Students say Osmosis is 100% worth it
Because Osmosis saves them time. Lowers stress. And actually helps them remember when it counts.
I used Osmosis to prepare for my first medical school licensing exam! Super helpful and interactive for people who may not do great with just pages of text info!
Cecilia Ruiz
MD student

I have used Osmosis for about four years. Best thing I have ever used for my medical studies.
Sayan Misra
Med student
Osmosis videos are superior because they define simple concepts, tell a story with a clear progression, and provide context.
Jay Pate
Dental student