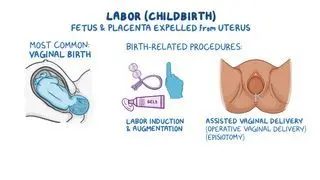
An episiotomy is an incision made at the perineum, the area between the vagina and the anus, in order to enlarge the vaginal opening during labor and delivery. Occasionally, the vaginal opening cannot stretch enough to accommodate the baby's head. In such cases, an episiotomy widens the vaginal opening and facilitates delivery. The American College of Obstetricians and Gynecologists (ACOG) recommends that episiotomies only be conducted when they are absolutely necessary, which includes situations where the fetus is stressed (e.g., low heart rate), the fetus is stuck behind the mother’s pelvic bone (e.g., shoulder dystocia), or to prevent larger tears. A surgical incision is preferred to a severe, uncontrolled perineal tear to minimize the risk of surrounding tissue damage (e.g., tearing of external and internal anal sphincters).
Once the placenta is delivered, the OBGYN may suture the incision. If the individual did not receive an epidural (i.e., a type of anesthesia that numbs sensation from the umbilicus to the upper legs) prior to labor, injection of a local anesthetic (e.g., xylocaine) into the perineum is typically required before suturing.
There are two types of episiotomies: median and mediolateral. The median episiotomy consists of a vertical incision, which is easier to repair but carries a higher risk of extending into the anal area and causing anal sphincter injury. The mediolateral incision, on the other hand, is done at an angle, typically at five or seven o’clock, and is less likely to extend to the anal region. However, a mediolateral incision is often more painful and difficult to repair. The tissues incised and later requiring suturing are the vaginal epithelium, pelvic floor muscles (including bulbocavernosus muscle and superficial and deep transverse perineal muscles), and perineal skin. In larger episiotomies, the ischiorectal fat may be exposed, and the external anal sphincter or levator ani may be partially cut.