
Today, we’re examining a clinical case of a 43-year-old man admitted to the ICU following an opiate overdose. What should be done next to identify the likely cause of his cyanosis and respiratory acidosis?
A 43-year-old man is admitted to the intensive care unit following an opiate overdose requiring intubation. The patient is mechanically ventilated and sedated on a propofol and fentanyl infusion. During rounds, the patient appears increasingly cyanotic. The patient has a history of alcoholism and opiate use disorder and does not take any medication daily. Temperature is 37°C (98.6°F), heart rate 115/min, blood pressure 136/68 mmHg, respiratory rate 10/min, and O2 saturation 93% on 100% FIO2. The patient is not over-breathing the ventilator. Bilateral breath sounds are present and cardiac examination is within normal limits. The patient has evidence of skin cyanosis. Stat blood gas results are obtained, which show pH 7.27 and a pCO2 50. A chest x-ray demonstrates that the endotracheal tube is 2 cm above the carina.
Which of the following should be assessed next to help determine the cause of cyanosis and respiratory acidosis in this patient?
A. Ventilator settings
B. Rate of fentanyl infusion
C. Ocular examination
D. Reflexes
E. Endotracheal tube placement via direct laryngoscopy
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
A. Ventilator settings
Correct: See Main Explanation.
Incorrect Answer Explanations
B. Rate of fentanyl infusion
Incorrect: This patient is intubated and mechanically ventilated with a set respiratory rate. The rate of fentanyl infusion will not affect the respiratory parameters and cause a low respiratory rate of 10 breaths/min which is most likely the cause of respiratory acidosis in this patient.
C. Ocular examination
Incorrect: An ocular examination is unlikely to provide useful information regarding the cause of respiratory acidosis in this patient who is sedated on propofol and fentanyl and has a low respiratory rate and raspatory acidosis.
D. Reflexes
Incorrect: Reflexes would not add additional information for this patient who is intubated and sedated with new cyanosis, respiratory acidosis, and a low respiratory rate.
E. Endotracheal tube placement via direct laryngoscopy
Incorrect: This patient has an endotracheal tube that is appropriately positioned on chest x-ray. Direct laryngoscopy is not necessary now and would not add more information. This patient should have the ventilatory settings checked and likely have the respiratory rate increased.
Main Explanation
This patient is intubated and sedated following respiratory failure secondary to opiate overdose. The patient has evidence of cyanosis on examination with confirmed proper placement of the endotracheal tube, and ABG results demonstrate respiratory acidosis. Given this clinical setting, iatrogenic causes of respiratory acidosis secondary to ventilation should be considered, such as low tidal volumes, low respiratory rate, and equipment failure. A fault in any one of these settings may result in hypercapnia and subsequent acidosis. This patient’s respiratory rate is most likely set too low given his RR of 10 breaths/min and likely resultant respiratory acidosis.
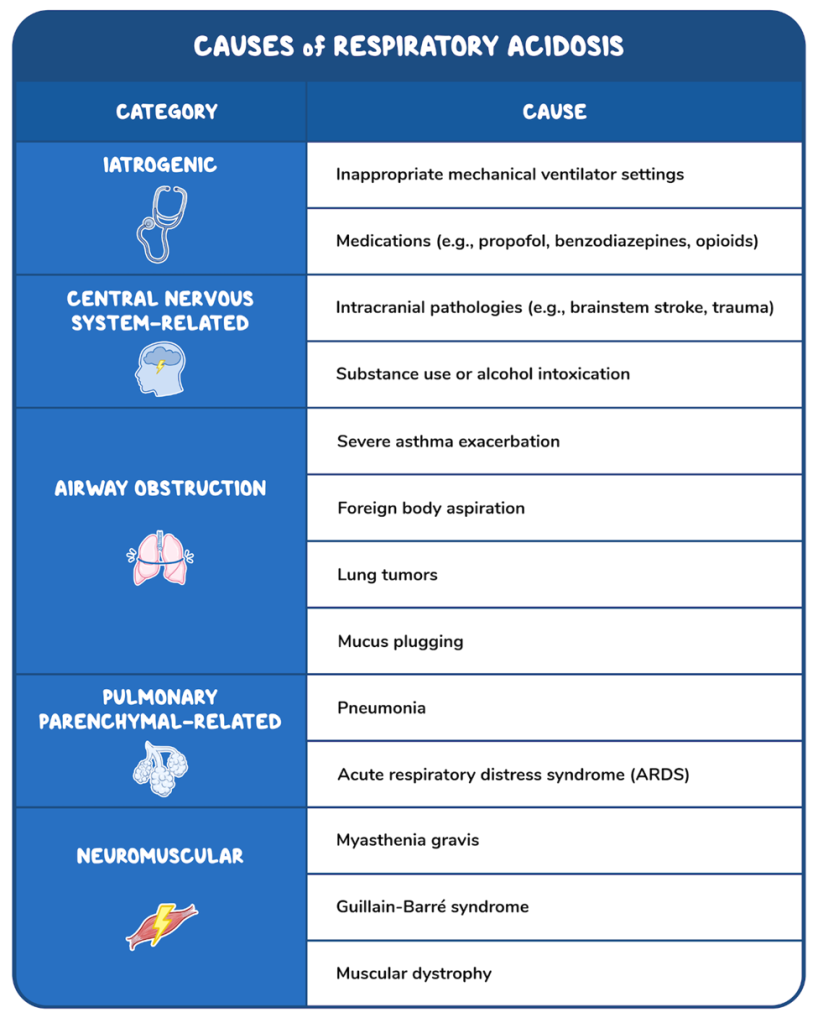
Many conditions fall can cause respiratory acidosis, including central nervous system (CNS), neuromuscular, obstructive, and parenchymal pulmonary etiologies; however, the presenting symptoms will be similar. Patients with respiratory acidosis may present with cyanosis, a decreased respiratory rate, or shortness of breath. Depending on the degree of hypercapnia, patients may also develop altered mental status and lethargy. Specific etiologies and appropriate treatments can be suggested by the clinical scenario–e.g., ventilated patients may need ventilator settings adjusted. Whereas patients with a focal neurologic deficit should have brain imaging to rule out CNS pathology (e.g., ICH).
Major Takeaway
Patients with respiratory acidosis tend to present with either cyanosis, a decreased respiratory rate, or shortness of breath. Mechanically ventilated patients with respiratory acidosis on ABG should have ventilator settings checked and equipment examined.
References
- (2019). Guidelines on diagnosis and treatment of CAP. ATS/IDSA.
- https://pubmed.ncbi.nlm.nih.gov/31573350
- (2015). Guideline for management of acute hypercapnic respiratory failure. BTS/ICS. https://doi.org/10.1136/thoraxjnl-2015-208209
- Metlay JP, Waterer GW, Long AC, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7): e45-e67. doi:10.1164/rccm.201908-1581ST
- Davidson AC, Banham S, Elliott M, et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults [published correction appears in Thorax. 2017 Jun;72 (6):588]. Thorax. 2016;71 Suppl 2: ii1-ii35. doi:10.1136/thoraxjnl-2015-208209
- Athayde RAB, Oliveira Filho JRB, Lorenzi Filho G, Genta PR. Obesity hypoventilation syndrome: a current review. J Bras Pneumol. 2018;44(6):510-518. doi:10.1590/S1806-37562017000000332
- Castro D, Patil SM, Keenaghan M. Arterial Blood Gas. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 12, 2022.
- Hillman D, Singh B, McArdle N, Eastwood P. Relationships between ventilatory impairment, sleep hypoventilation and type 2 respiratory failure. Respirology. 2014;19(8):1106-1116. doi:10.1111/resp.12376
- Pisani L, Corcione N, Nava S. Management of acute hypercapnic respiratory failure. Curr Opin Crit Care. 2016;22(1):45-52. doi:10.1097/MCC.0000000000000269
- Qadir N, Sahetya S, Munshi L, et al. An Update on Management of Adult Patients with Acute Respiratory Distress Syndrome: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2024;209(1):24-36. doi:10.1164/rccm.202311-2011ST Shigemura M, Lecuona E, Sznajder JI. Effects of hypercapnia on the lung. J Physiol. 2017;595(8):2431-2437. doi:10.1113/JP273781

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning with us.
Leave a Reply