
This week, we are sharing another PANCE®-style practice question to test your knowledge of medical topics. Today’s case focuses on a 49-year-old man with cirrhosis and vomiting blood. Explore his symptoms, physical examination findings, and lab results to determine the most appropriate treatment. Learn more about this critical medical scenario.
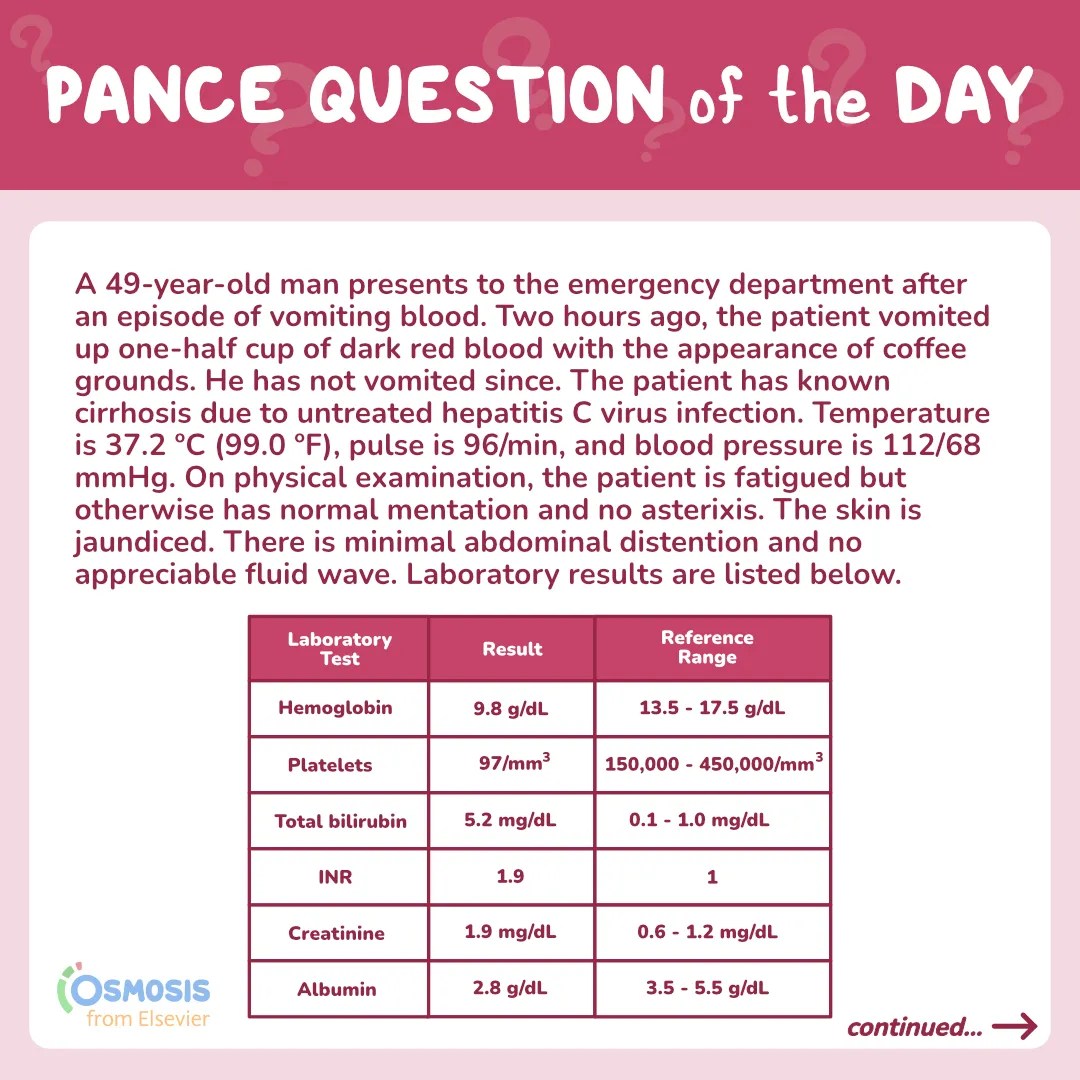
A 49-year-old man presents to the emergency department after an episode of vomiting blood. Two hours ago, the patient vomited up one-half cup of dark red blood with the appearance of coffee grounds. He has not vomited since. The patient has known cirrhosis due to untreated hepatitis C virus infection. Temperature is 37.2 ºC (99.0 ºF), pulse is 96/min, and blood pressure is 112/68 mmHg. On physical examination, the patient is fatigued but otherwise has normal mentation and no asterixis. The skin is jaundiced. There is minimal abdominal distention and no appreciable fluid wave. Laboratory results are listed below. Which of the following is the most appropriate treatment?
| Laboratory Test | Result | Reference Range |
| Hemoglobin | 9.8 g/dL | 13.5 – 17.5 g/dL |
| Platelets | 97/mm3 | 150,000 – 450,000 / mm3 |
| Total bilirubin | 5.2 mg/dL | 0.1 – 1.0 mg/dL |
| INR | 1.9 | 1.0 |
| Creatinine | 1.9 mg/dL | 0.6 – 1.2 mg/dL |
| Albumin | 2.8 g/dL | 3.5 – 5.5 g/dL |
A. Ceftriaxone
B. Packed red blood cells
C. Lactulose
D. Sofosbuvir-velpatasvir
E. Albumin
Scroll down for the correct answer!
The correct answer to today’s PANCE® Question is…
A. Ceftriaxone
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect answer explanations
B. Packed red blood cells
Incorrect: This patient’s hemoglobin is adequate and transfusion of packed red blood cells is unnecessary at this time. Transfusion would be appropriate if the patient’s hemoglobin was < 7 g/dL or if it was 7-8 g/dL and the patient had severe ongoing hemorrhage.
C. Lactulose
Incorrect: Lactulose is important for treating and preventing hepatic encephalopathy in patients with cirrhosis. This patient’s mentation is appropriate and treating the acute issues takes precedence.
D. Sofosbuvir-velpatasvir
Incorrect: This medication is indicated for treating chronic hepatitis C virus infection. This treatment would be appropriate once the patient is no longer acutely ill.
E. Albumin
Incorrect: There are specific indications for the use of albumin in patients with cirrhosis, such as hepatorenal syndrome or large-volume paracentesis. This patient has adequate blood pressure and would not benefit from an albumin infusion.

Main Explanation
This patient with untreated hepatitis C infection and resultant cirrhosis presents with an acute upper GI bleed (e.g. variceal bleed, peptic ulcer disease). In patients with cirrhosis who present with an upper GI bleed, empiric antibiotics (e.g. ceftriaxone) should be started since these patients are at significant risk of resultant infection, such as spontaneous bacterial peritonitis. Lactulose should be given if there is evidence of hepatic encephalopathy, and the abdomen should be evaluated for ascites, which may require paracentesis.

Hepatitis C virus (HCV) is a bloodborne infection transmitted via exposure to contaminated blood or through sexual contact. It typically causes an asymptomatic acute infection. If the infection is not cleared, it can lead to chronic infection which predisposes the patient to cirrhosis and hepatocellular carcinoma. Hepatitis C should be suspected in patients with known high-risk behaviors or exposures (e.g., tattooing with non-sterile equipment, IV drug use, sexual contact with a known HCV carrier). It should also be part of the differential diagnosis for patients presenting with jaundice, abdominal pain, anorexia, and other symptoms of liver damage.
When HCV is suspected, serum HCV antibody testing should be performed. If positive, serum HCV RNA should then be tested to determine if this is an old, resolved infection or an active infection. Patients with active infection (positive HCV RNA) should be treated with antivirals, such as sofosbuvir-velpatasvir or glecaprevir-pibrentasvir. Patients should be counseled about lifestyle modifications (e.g. alcohol cessation) and vaccinated against hepatitis A and B virus. If HCV RNA is negative and there is a high suspicion of infection, HCV RNA testing should be repeated in six months. If HCV RNA is still negative at that point, then the HCV antibody was likely a false positive.
Major Takeaway
Acute management for patients with an HCV infection may include treatment of complications related to cirrhosis or fulminant liver failure. This may include therapies aimed at treating variceal bleeding (e.g., blood products, ceftriaxone), hepatic encephalopathy (e.g. lactulose), and ascites (e.g. paracentesis).
References:
Chavez-Tapia NC, Barrientos-Gutierrez T, Tellez-Avila F, Soares-Weiser K, Mendez-Sanchez N, Gluud C, Uribe M. Meta-analysis: antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding – an updated Cochrane review. Aliment Pharmacol Ther. 2011 Sep;34(5):509-18. doi: 10.1111/j.1365-2036.2011.04746.x. Epub 2011 Jun 27. PMID: 21707680.
European Association for the Study of the Liver. Electronic address: [email protected]. EASL Recommendations on Treatment of Hepatitis C 2016. J Hepatol 2017; 66:153.
HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Joint panel from the American Association of the Study of Liver Diseases and the Infectious Diseases Society of America. http://www.hcvguidelines.org/ (Accessed on May 2, 2023).
________________________
Leave a Reply