
This week, we’re sharing another USMLE® Step 1-style practice question about a 66-year-old person with shortness of breath with exertion. What’s the pathophysiology of this patient’s pulmonary findings?
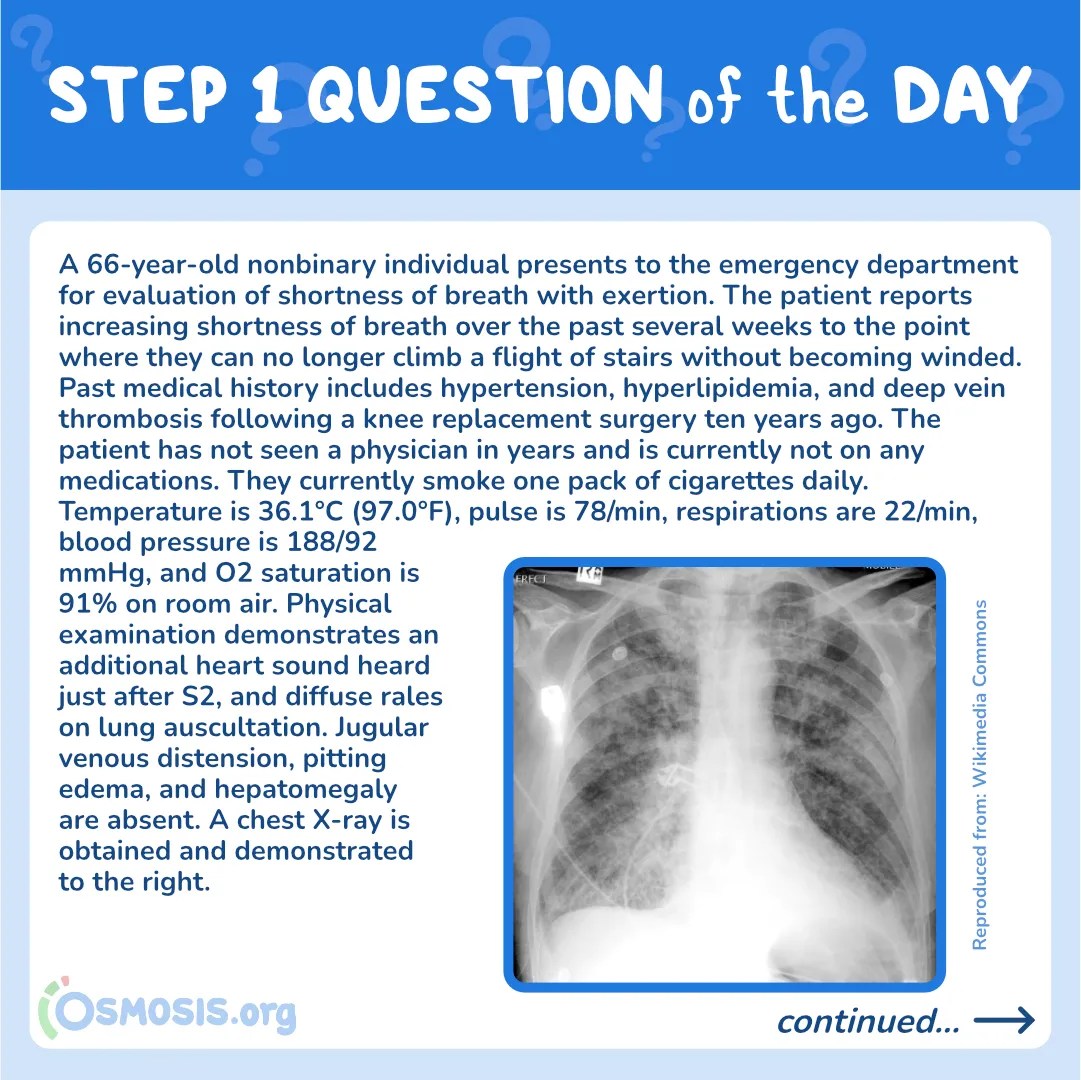
A 66-year-old nonbinary individual presents to the emergency department for evaluation of shortness of breath with exertion. The patient reports increasing shortness of breath over the past several weeks to the point where they can no longer climb a flight of stairs without becoming winded. Past medical history includes hypertension, hyperlipidemia, and deep vein thrombosis following a knee replacement surgery ten years ago. The patient has not seen a physician in years and is currently not on any medications. They currently smoke one pack of cigarettes daily. Temperature is 36.1°C (97.0°F), pulse is 78/min, respirations are 22/min, blood pressure is 188/92 mmHg, and O2 saturation is 91% on room air. Physical examination demonstrates an additional heart sound heard just after S2, and diffuse rales on lung auscultation. Jugular venous distension, pitting edema, and hepatomegaly are absent. A chest X-ray is obtained and demonstrated below.
Which of the following best describes the pathophysiology of this patient’s pulmonary findings?

A. Increased pulmonary venous pressure
B. Decreased pulmonary venous pressure
C. Increased central venous pressure
D. Decreased pulmonary capillary wedge pressure
E. Recurrent pulmonary embolism
Scroll down to find the answer!
The correct answer to today’s USMLE® Step 1 Question is…
A. Increased pulmonary venous pressure
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect Answer Explanations
B. Decreased pulmonary venous pressure
Incorrect: Increased, not decreased, pulmonary venous pressure likely underlies this patient’s pulmonary findings. With left-sided heart failure, poor ejection fraction manifests with increased pulmonary capillary wedge pressure, increased pulmonary venous pressure, and subsequent transudation of fluid into the lung parenchyma.
C. Increased central venous pressure
Incorrect: Increased central venous pressure occurs in the setting of right heart failure. Right heart failure can manifest with pitting edema, hepatosplenomegaly, and jugular venous distension. In contrast, these findings are absent in this patient.
D. Decreased pulmonary capillary wedge pressure
Incorrect: Increased, not decreased, pulmonary capillary wedge pressure leads to the development of pulmonary edema.
E. Recurrent pulmonary embolism
Incorrect: While this patient has a history of a remote deep vein thrombosis, he has no evidence of right heart failure on examination. This patient’s pulmonary findings are more likely secondary to left-sided heart failure and a different underlying etiology.

Main Explanation
This patient presents with clinical features consistent with left-heart failure including an S3 gallop and pulmonary edema. The primary pathophysiology underlying pulmonary edema secondary to left-sided heart failure is an increase in pulmonary venous pressure and subsequent transudation of fluid into the lung parenchyma.
Left-sided heart failure refers to the anatomical failure of the left side of the heart only and presents with characteristic symptoms and examination findings. Notably, patients present with orthopnea (shortness of breath when lying supine), paroxysmal nocturnal dyspnea (breathless awakening from sleep), and pulmonary edema. The former two findings are largely due to increased venous return and redistribution of blood when lying flat, whereas pulmonary edema results from impaired forward arterial blood flow and vascular congestion.

Major Takeaway
Left-sided heart failure refers to dysfunction of the left heart. The condition results in clinical features including orthopnea, paroxysmal nocturnal dyspnea, and pulmonary edema.
References
- Kumar, V., Abbas, A.K., Aster, J.C., Perkins, J.A., Robbins, S.L. (2018) Robbins basic pathology (10th ed.). Philadelphia, PA: Elsevier. ISBN: 978-0323353175.
- Luk, A., Ahn, E., Soor, G.S., Butany, J. (2009) Dilated cardiomyopathy: A review. Journal of Clinical Pathology. 62(3), 219‐225. Doi:10.1136/jcp.2008.060731.
- Veselka, J., Anavekar, N.S., Charron, P. (2017) Hypertrophic obstructive cardiomyopathy. Lancet. 389(10075), 1253-1267. Doi: 10.1016/S0140-6736(16)31321-6.
- Yancy, C.W., Jessup, M., Bozkurt, B., et al. (2013) 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 62(16), e147-e239. Doi: 10.1161/CIR.0b013e31829e8807.

Want more USMLE® Step 1 practice questions? Try Osmosis from Elsevier today! Access your free trial and find out why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply