
We’re back with a USMLE® Step 2 CK Question of the Day! Today’s case involves an 18-year-old woman with a history of type 1 diabetes mellitus who complains of nausea and flank pain. Can you figure it out? Let’s find out!
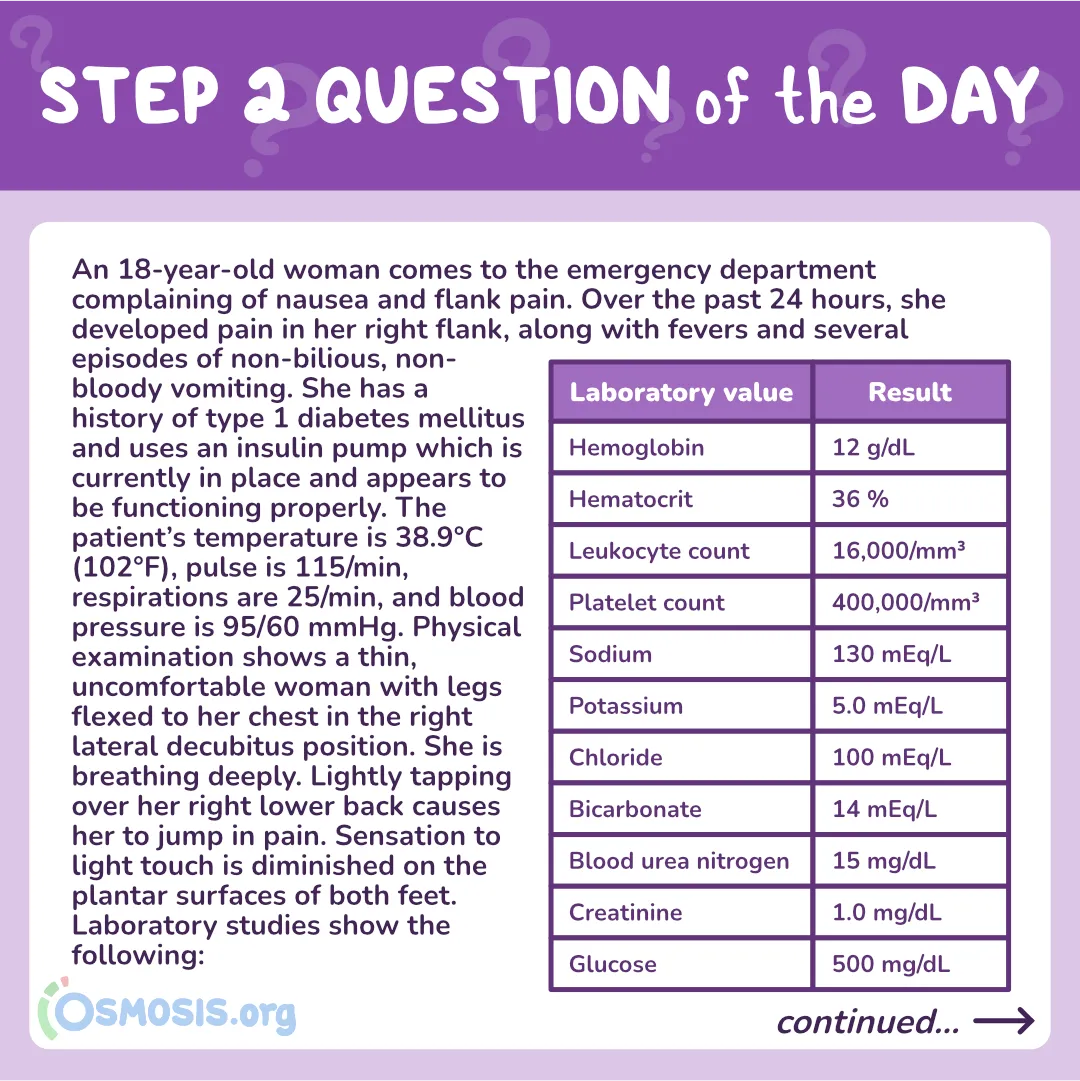
An 18-year-old woman comes to the emergency department complaining of nausea and flank pain. Over the past 24 hours, she developed pain in her right flank, along with fevers and several episodes of non-bilious, non-bloody vomiting. She has a history of type 1 diabetes mellitus and uses an insulin pump which is currently in place and appears to be functioning properly. The patient’s temperature is 38.9°C (102°F), pulse is 115/min, respirations are 25/min, and blood pressure is 95/60 mmHg. Physical examination shows a thin, uncomfortable woman with legs flexed to her chest in the right lateral decubitus position. She is breathing deeply. Lightly tapping over her right lower back causes her to jump in pain. Sensation to light touch is diminished on the plantar surfaces of both feet. Laboratory studies show the following:
| Laboratory value | Result |
| Hemoglobin | 12 g/dL |
| Hematocrit | 36 % |
| Leukocyte count | 16,000/mm3 |
| Platelet count | 400,000/mm3 |
| Sodium | 130 mEq/L |
| Potassium | 5.0 mEq/L |
| Chloride | 100 mEq/L |
| Bicarbonate | 14 mEq/L |
| Blood urea nitrogen | 15 mg/dL |
| Creatinine | 1.0 mg/dL |
| Glucose | 500 mg/dL |
Which of the following solutes is most important to replenish at this point in time?
A. Sodium
B. Potassium
C. Chloride
D. Bicarbonate
E. Glucose
Scroll down for the correct answer!
Check out our free USMLE® Step 2 Ultimate Guide!
The correct answer to today’s USMLE® Step 2 CK Question is…
B. Potassium
Before we get to the Main Explanation, let’s see why the answer wasn’t A, C, D or E. Skip to the bottom if you want to see the correct answer right away!
Incorrect Answer Explanations
A. Sodium
Incorrect: An increase in extracellular glucose concentration moves water out of cells, causing dilution of extracellular sodium and a falsely low serum sodium level on lab values. For every 100 mg/dL of glucose over 100, you can expect a 1.6 drop in sodium. This patient’s corrected sodium level is normal at 136 mEq/L.
C. Chloride
Incorrect: Serum chloride levels are usually normal in patients with diabetic ketoacidosis and do not require focused repletion beyond what is given in isotonic fluids.
D. Bicarbonate
Incorrect: Although this patient’s bicarbonate is low, indicating diabetic ketoacidosis, the proper way to fix it is by treating the underlying cause with insulin and intravenous fluids. Clinical trials do not support the routine use of bicarbonate replacement in diabetic ketoacidosis.
E. Glucose
Incorrect: Treating diabetic ketoacidosis requires insulin to allow the body to process all of the built up extracellular glucose. Only once the plasma glucose reaches 200-250 mg/dL is glucose added to the insulin infusion to prevent massive drops in serum glucose, which can cause cerebral edema.
Main Explanation
This patient is presenting with signs and symptoms of pyelonephritis in the setting of well-controlled type 1 diabetes mellitus with evidence of chronic peripheral neuropathy (extremity numbness). Pyelonephritis, or an infection of the kidney, is more common in diabetic patients and causes nausea, vomiting, fever, leukocytosis, and flank pain with costovertebral tenderness on physical examination. Although this patient’s diabetes has stably been controlled on her insulin pump, infections increase the body’s insulin requirement and are thus a common trigger for diabetic ketoacidosis (DKA). Without any insulin, lipolysis occurs and the liver starts to turn fatty acids into ketone bodies, such as aceto-acetic acid and beta hydroxybutyric acid, thereby increasing the acidity of the blood, causing an anion-gap metabolic acidosis.

Clinically, individuals with DKA are dehydrated from hyperglycemic polyuria. The acidosis causes Kussmaul respiration, which is deep and rapid breathing as the body tries to move carbon dioxide out of the blood to reduce its acidity. Abdominal pain, nausea, vomiting, and mental status changes like delirium and psychosis can occur. Laboratory results show hyperglycemia with low serum pH and low bicarbonate. The anion gap is high, which reflects a large difference in the unmeasured negative and positive ions in the serum, largely due to this build-up of ketoacids.
Potassium is critically important to replete in DKA. Recall that cells have a transporter that exchanges hydrogen ions for potassium. When the blood gets acidic, there are many positively charged hydrogen ions present in the blood. Cells will exchange these extracellular protons with intracellular potassium, so initially there will be hyperkalemia. In addition to helping glucose enter cells, insulin also stimulates the sodium-potassium ATPases that help potassium get into cells; without insulin, more potassium stays in the extracellular fluid. Since this extracellular potassium is quickly excreted, even though the blood potassium levels remain high, total body potassium is depleted. Therefore, treatment of DKA relies on IV fluids to correct dehydration, IV insulin to reverse lipolysis, and aggressive potassium repletion as soon as serum potassium levels are in the normal range.
Major Takeaway
Diabetic ketoacidosis can occur in patients with type 1 diabetes if they are stressed or have missed insulin doses. Laboratory studies show an anion-gap metabolic acidosis with hyperglycemia causing spuriously low sodium levels. Acidemia with extracellular potassium wasting results in depleted total body potassium stores, even though the blood level may be normal or elevated, and potassium repletion should begin immediately.
Want to learn more about this topic?
Watch this Osmosis video: Diabetic ketoacidosis: Clinical sciences
References
- Powers, A. C., Niswender, K. D., & Rickels, M. R. (2018). Diabetes Mellitus: Management and Therapies. In J. L. Jameson, A. S. Fauci, D. L. Kasper, S. L. Hauser, D. L. Longo, & J. Loscalzo (Eds.), Harrison’s Principles of Internal Medicine (20th ed.). McGraw-Hill Education.

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Get your free trial and find out why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply