
A 60-year-old man, who’s been feeling off-balance and experiencing several near-falls, arrives at his PCP clinic. What’s the most likely cause of his unsteadiness? Let’s find out!
A 60-year-old man presents to the primary care clinic for evaluation of frequent falls. For the past year, the patient has felt increasingly unsteady, and for the past six months has had several near-falls. The patient feels even more unsteady in the dark or when his eyes are closed. Past medical history includes hypertension, which is well-controlled with lisinopril. Temperature is 37.0°C (98.6°F), pulse is 84/min, respirations are 14/min, and blood pressure is 110/75 mmHg. On physical examination, the patient’s gait is wide-based with forceful stepping. Dimming the lights while the patient walks causes more unsteadiness. Serum hemoglobin A1c and vitamin B12 levels are normal.
Which of the following diagnostic tests is most likely to confirm the diagnosis?
A. PMP22 gene duplication
B. Serologic and cerebrospinal fluid (CSF) syphilis testing
C. Frataxin gene mutation with expanded GAA repeats
D. Magnetic resonance imaging (MRI) of the cervical spine
E. Magnetic resonance imaging (MRI) of the brain
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
B. Serologic and cerebrospinal fluid (CSF) syphilis testing
Correct: See Main Explanation.
Incorrect Answer Explanations
A. PMP22 gene duplication
Incorrect: This patient presents with a stomping gait pattern (i.e., wide-based, unsteady, forceful steps) rather than the steppage gait pattern (i.e., excessive hip flexion, high steps, foot drop) associated with Charcot-Marie-Tooth disease. Given the normal hemoglobin A1c and vitamin B12 levels, tabes dorsalis should be considered; this can be confirmed through serologic and CSF testing for syphilis.
C. Frataxin gene mutation with expanded GAA repeats
Incorrect: This patient presents with a stomping gait pattern (i.e., wide-based, unsteady, forceful steps) rather than the ataxic gait pattern (i.e., wide-based, veering to the side, irregular rhythm, and stride length) associated with Friedreich ataxia. Given the normal hemoglobin A1c and vitamin B12 levels, tabes dorsalis should be considered; this can be confirmed through serologic and CSF testing for syphilis.
D. Magnetic resonance imaging (MRI) of the cervical spine
Incorrect: This patient presents with a stomping gait pattern, which can be associated with tabes dorsalis, vitamin B12 deficiency, or diabetic neuropathy. Given the normal hemoglobin A1c and vitamin B12 levels, tabes dorsalis should be considered; this can be confirmed through serologic and CSF syphilis testing. Imaging of the spine can sometimes show longitudinal hyperintensities in the dorsal columns, but this finding is neither sensitive nor specific for tabes dorsalis.
E. Magnetic resonance imaging (MRI) of the brain
Incorrect: This patient presents with a stomping gait pattern, which can be associated with tabes dorsalis, vitamin B12 deficiency, or diabetic neuropathy. Brain imaging is not diagnostic for these causes. Because this patient’s hemoglobin A1c and vitamin B12 levels were normal, serologic and CSF testing for syphilis are indicated to evaluate for tabes dorsalis.
Main Explanation
This patient presents with unsteadiness, frequent falls, and a stomping gait pattern characterized by forceful, wide-based steps that worsens in low light. In the absence of diabetes mellitus or vitamin B12 deficiency, tabes dorsalis is the most likely diagnosis. On magnetic resonance imaging (MRI), longitudinal T2 hyperintensities in the posterior spinal cord may be seen, but these findings are neither sensitive nor specific. The most definitive evidence comes from positive syphilis serology and a reactive VDRL in the cerebrospinal fluid.
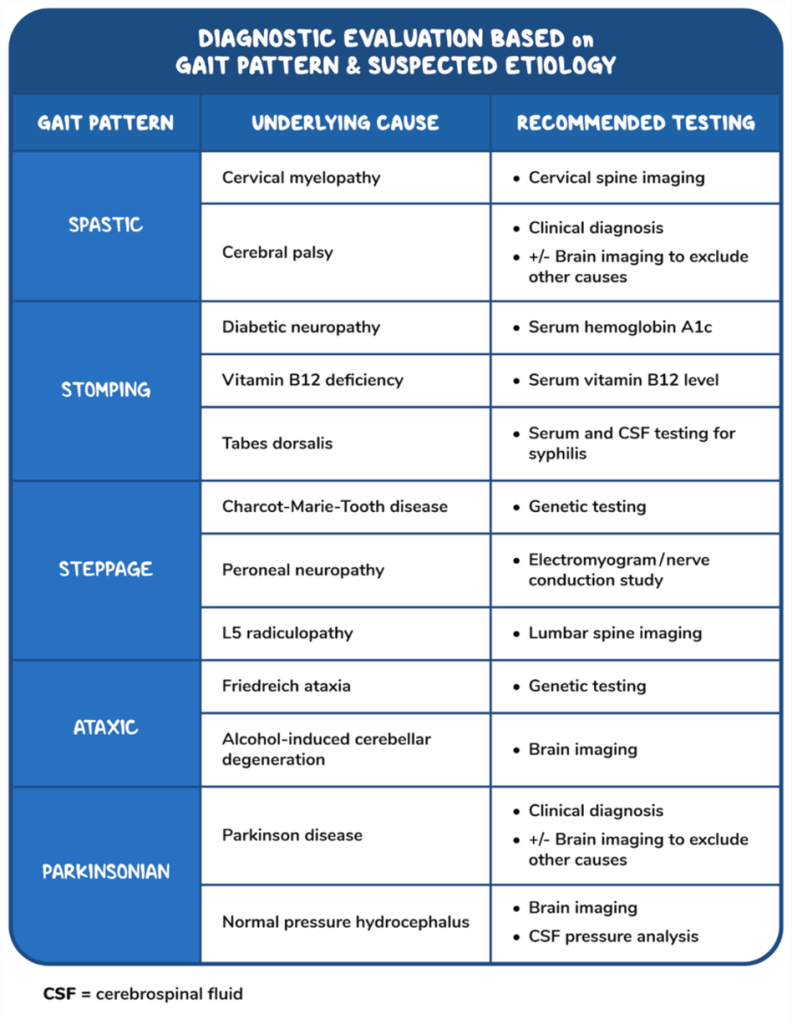
Patients may experience gait dysfunction because of motor weakness, sensory loss, poor coordination, or movement disorders. These issues can result in various gait patterns, including spastic, stomping, steppage, ataxic, and Parkinsonian gait. Assessing the pattern of gait dysfunction helps narrow the differential diagnosis and direct further diagnostic testing, such as imaging studies, genetic testing, laboratory tests, and electromyography and nerve conduction studies. The table above provides more detailed guidance on next steps based on suspected etiology.
Major Takeaway
A stomping gait pattern occurs in tabes dorsalis, vitamin B12 deficiency, and diabetic polyneuropathy. Tabes dorsalis can be confirmed with serologic and cerebrospinal fluid testing for syphilis.
Want to learn more about this topic?
Watch the Osmosis video: Approach to unsteadiness, gait disturbance, or falls: Clinical sciences
References
- Papp, J.R. et al. (8 February 2024). CDC Laboratory Recommendations for Syphilis Testing, United States, 2024. Morbidity and Mortality Weekly Report 73(1): 1-32.

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply