
A patient with a history of HIV presents with a worsening headache , neck stiffness, light senstivity, and occasional fever over the past two weeks. Which of the following is the most likely diagnosis?
A 53-year-old man presents to the emergency department for evaluation of headache. For the past two weeks, the patient has experienced a gradually intensifying, constant headache with associated light sensitivity and neck stiffness. The patient has a medical history significant for HIV, and he has been non-adherent with antiretroviral agents. On review of systems, the patient has had intermittent fever and cough. The patient does not currently take any medications. Temperature is 39.0°C (102.2°F), pulse is 110/min, respirations are 22/min, and blood pressure is 130/85 mmHg. On physical examination, the patient is squinting and resisting passive movement of the neck. With forward flexion of the neck, the hips flex bilaterally. A lumbar puncture is performed; results are shown below.
| Cerebrospinal fluid (CSF) analysis | Result |
| Appearance | Clear |
| Glucose | 60 mg/dL |
| Protein | 70 mg/dL |
| White blood cell count | 450/microL |
| Red blood cell count | 0/microL |
| Opening pressure | 30 cmH2O |
| India ink stain | Positive |
| Acid-fast stain | Negative |
Which of the following is the most likely causative organism in this patient’s condition?
A. Cryptococcus neoformans
B. Streptococcus pneumoniae
C. Listeria monocytogenes
D. Herpes simplex virus
E. Mycobacterium tuberculosis
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
A. Cryptococcus neoformans
Correct: See Main Explanation.
Incorrect Answer Explanations
B. Streptococcus pneumoniae
Incorrect: Bacterial meningitis typically features a very high CSF white blood cell count (>1,000/microL), low glucose, and high protein (>100 mg/dL). In contrast, this case features a lower WBC count (450/microL), normal glucose, and only mildly elevated protein (70 mg/dL), along with positive India ink staining; this profile is more suggestive of cryptococcal meningitis.
C. Listeria monocytogenes
Incorrect: Bacterial meningitis typically features a very high CSF white blood cell count (>1,000/microL), low glucose, and high protein (>100 mg/dL). In contrast, this case features a lower WBC count (450/microL), normal glucose, and only mildly elevated protein (70 mg/dL), along with positive India ink staining; this profile is more suggestive of cryptococcal meningitis.
D. Herpes simplex virus
Incorrect: Viral meningitis typically features a slightly higher CSF white blood cell count (up to 1,000/microL) and the presence of red blood cells (RBCs). In contrast, the lower WBC count (450/microL), positive India ink staining, and lack of RBCs in this patient’s CSF profile are more suggestive of cryptococcal meningitis.
E. Mycobacterium tuberculosis
Incorrect: Tuberculous meningitis typically features low glucose in the CSF, in addition to a positive acid-fast test. In contrast, the normal glucose and positive India ink staining in this case are more suggestive of cryptococcal meningitis.
Main Explanation

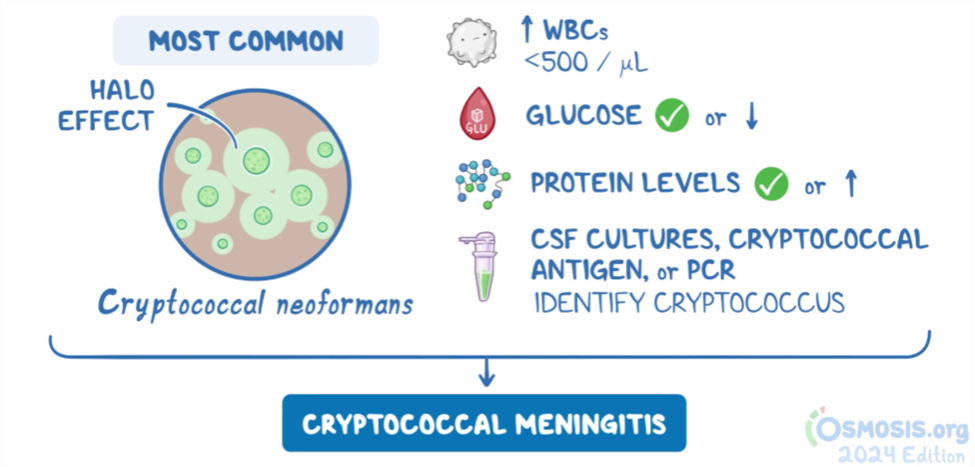
This immunocompromised patient presents with signs and symptoms of cryptococcal meningitis, including fever, headache, neck stiffness, and light sensitivity. The subacute presentation is typical of cryptococcal meningitis, which is most common in patients with a CD4 count <100 cells/microL. The CSF white blood cell (WBC) count is often elevated but typically not exceeding 500 cells/microL. Glucose levels are usually slightly low or normal, protein levels may be normal or elevated, and opening pressure is often high. A positive India ink stain is key in distinguishing this from other forms of meningitis.
In tuberculous meningitis, CSF analysis may show a similar WBC count and glucose and protein levels, but the India ink stain will be negative, and an acid-fast stain will be positive. Non-tuberculous bacterial meningitis typically features a very high WBC count with a neutrophilic predominance, low glucose, and elevated protein. Viral meningitis shows a variable WBC count with a lymphocytic predominance, normal or slightly low glucose, and normal or slightly elevated protein. In herpes simplex virus (HSV) meningitis, the red blood cell count may be significantly elevated even with a non-traumatic lumbar puncture.
Major Takeaway
Cryptococcal meningitis should be suspected in individuals with potentially advanced HIV, and it can be differentiated from other forms of infectious meningitis through CSF analysis, which typically shows a moderately elevated (<500/microL), lymphocyte-predominant WBC count, normal or slightly low glucose, and normal or slightly elevated protein. Positive India ink staining is diagnostic.
Want to learn more about this topic?
Watch the Osmosis video: Meningitis and brain abscess: Clinical sciences
References
- Paramitha, P. and Ritarwan, K. (2022). Case Report: Cryptococcal Meningitis. Open Access Macedonian Journal of Medical Sciences 10(T7): 138-141.
- Pruitt, A.A. (26 May 2021). Central Nervous System Infections in Immunocompromised Patients. Current Neurology and Neuroscience Reports 21(7):1-10.

Get your free trial and discover why millions of current and future clinicians and caregivers love learning with us.
Leave a Reply