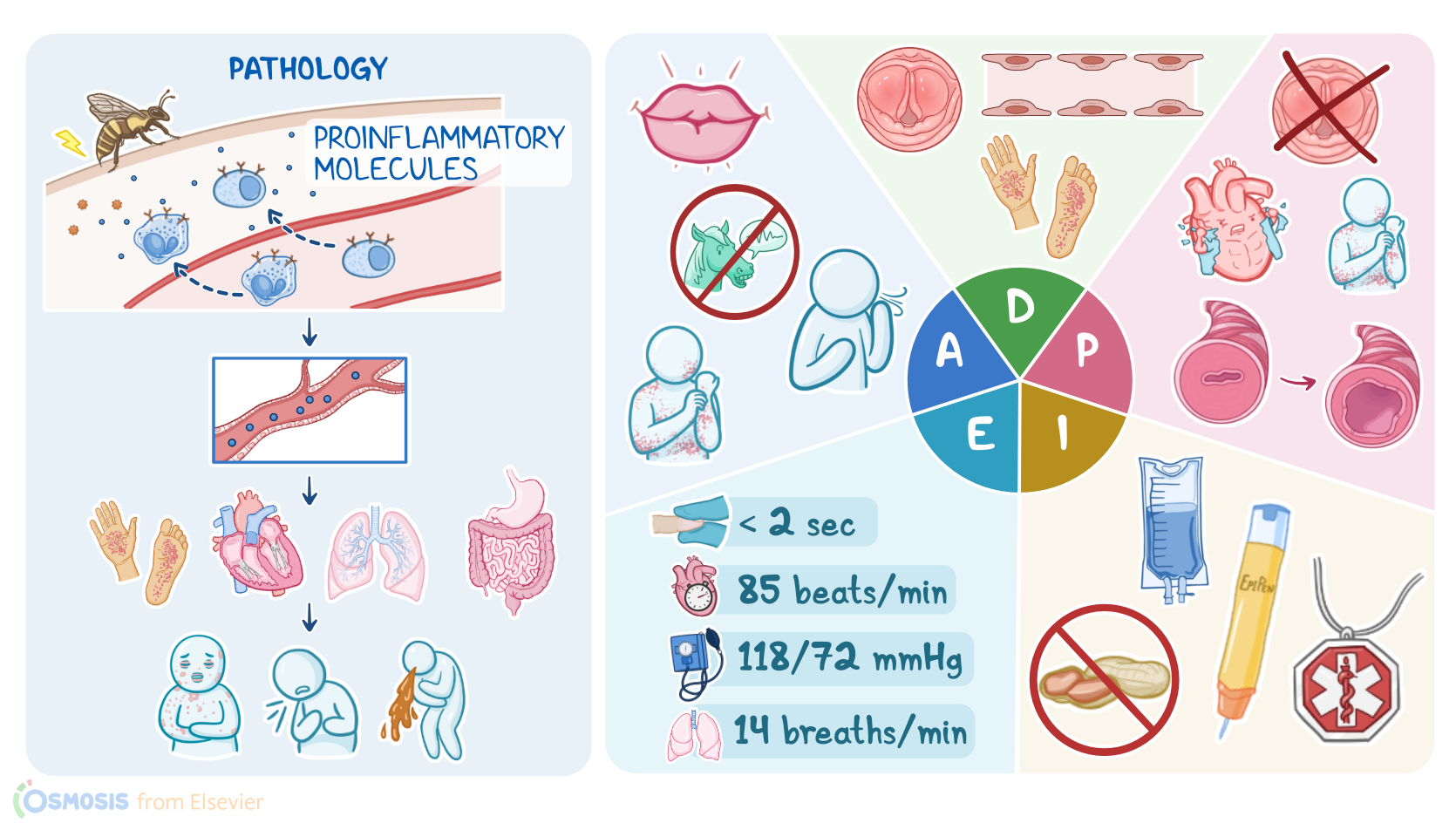
Anaphylaxis: Nursing process (ADPIE)
Client Report0:00–1:04
Jocelyn Williams is an 18 year old female client with a history of severe peanut allergy, who was brought to the emergency department, or ED via paramedics after accidentally eating a cookie that contained peanuts.
After a few bites, she felt a tingling sensation in her mouth and lips, and her tongue started to swell. She could not find her EpiPen, so her roommate called 911.
Upon arrival to the ED, the paramedic reports that Jocelyn's face was flushed and swollen at the time of their arrival. She had generalized hives, tachypnia, and labored respirations.
Her initial vital signs were tympanic temperature 98.7 °F or 37 °C, heart rate 126 BPM, respiratory rate 32 breaths per minute with audible wheezing, BP 96/60, and SPO2, 87% on room air.
They administered one dose of epinephrine IM per protocol, and placed her on a non-rebreather mask at 10 L per minute. Anaphylaxis is a severe allergic reaction that affects multiple organ systems and can be life-threatening.
Pathology1:04–6:30
Now, allergic reactions typically happen when the immune system overreacts and starts targeting harmless antigens that don't cause any problems for most people.
Other antigens include certain medications, such as antibiotics like penicillin, as well as NSAIDs or streptokinase, which is used as a thrombolytic therapy.
In addition, some clients can develop allergic reactions when exposed to latex or radiocontrast agents used for imaging techniques like a CT scan or MRI.
Now, let's say a person gets stung by a bee for the first time. So, the first time these antigens enter the body, they get picked up and recognized by immune cells called dendritic cells.
These then activate other immune cells, the T lymphocytes, which in turn stimulate B lymphocytes to secrete IgE antibodies into the bloodstream.
IgEs then bind to the surface of mast cells and basophils, which are immune cells that are full of granules that contain pro-inflammatory molecules like histamine.
Later on, if the same person gets stung by a bee again, their mast cells and basophils, which already have IGE antibodies on their surface, are able to recognize the antigens and release their pro-inflammatory molecules, triggering an allergic reaction.
In most cases, this would cause some localized damage, like a swelling around the sting site. But sometimes things get really serious, and there's massive release of pro-inflammatory molecules into the bloodstream.
When the allergic reaction involves two or more organ systems, such as the cutaneous, respiratory, cardiovascular, and gastrointestinal systems, it's called anaphylaxis.
Now, there are some factors that may put the client at risk of anaphylaxis, such as adipe, which means having a genetic predisposition to allergic reactions, including allergic rhinitis, asthma, and atopic dermatitis.
Other risk factors include having a personal or family history of anaphylaxis. Symptoms of anaphylaxis typically start right after exposure to the antigen, and usually peak within 30 minutes.
These include angioedema, where tissues all over the body might start to swell up, including the eyes, mouth, tongue, and throat.
Angioedema is often associated with cutaneous manifestations like urticaria, which presents with a skin rash and pruritis, as well as flushing of the skin.
Anaphylaxis can also cause respiratory symptoms like chest tightness, shortness of breath, coughing, and wheezing, as well as gastrointestinal symptoms like abdominal pain, vomiting, and diarrhea.
Now, if not promptly treated, anaphylaxis can progress to serious complications, like laryngeal edema, which can cause upper airway obstruction and even respiratory arrest.
In some cases, the massive release of pro-inflammatory molecules can lead to widespread vasodilation, which results in severe hypotension.
If BP gets so low that it can't supply vital organs like the heart or brain, it's called anaphylactic shock. Reduced blood supply to the heart could cause myocardial infarction, especially in clients who already have an underlying heart disease.
Well, reduced blood supply to the brain can cause loss of consciousness. Finally, if not promptly treated, anaphylaxis can lead to death.
Diagnosis of anaphylaxis is typically based on history and physical examination, as well as identifying a likely exposure and trigger.
One way to identify an allergic trigger is through skin prick tests, where small drops of allergens are pricked into the skin with a tool to see if there's evidence of an allergic reaction, like raised, itchy red bumps or wheels.
Finally, specific lab tests like histamine and IgE levels are usually elevated. Now, anaphylaxis is a medical emergency that needs immediate treatment, starting by ensuring a patent airway.
Next, epinephrine should be administered, most often intramuscularly, in the anterolateral thigh. Epinephrine causes blood vessel constriction, which decreases edema and increases BP.
Epinephrine also boosts the heart's contractility and heart rate, which can help prevent cardiovascular collapse. And finally, it relaxes the smooth muscles that line the bronchi, helping the airways to open up.
In case of anaphylactic shock, large amounts of intravenous fluids and vasopressors should be given. Once the client is stabilized, other medications can be given, such as oral or IV antihistamines, like diphenhydramine, as well as IV corticosteroids, like methylprednisolone and inhaled bronchodilators, like the beta-2-ag agonist albuterol.
In some cases, anaphylaxis can recur hours later without additional exposure to the allergen, known as biphasic anaphylaxis.
Because of that, clients should stay under close monitoring for at least a day after symptoms resolve, in case there's a biphasic reaction and another wave of symptoms.
OK, let's get back to assess Jocelyn and see how she's doing. She appears calm, and her voice is clear, and no hoarseness is noted.
Assessment6:30–7:28
Her lips remain swollen, but she says she feels like her tongue is getting smaller. She has generalized hives and is scratching her neck and chest.
Some expiratory wheezing is present, though her respirations are unlabored. Capillary refill is 3 seconds, with 2+ peripheral pulses.
Her vital signs are temporal temperature 98.8 °F or 37.1 °C, heart rate, 112 BPM, respiratory rate, 16 breaths per minute, BP 103/70 millimeters of mercury, SPO2 100% on 10 L per minute non-rebreather mask, and pain, 0 out of 10.
You document your assessment findings, share the information with the physician, and begin to develop a care plan for Jocelyn.
Diagnosis7:28–7:50
Based on the assessment data you collected, your nursing diagnoses include risk for decreased cardiac output related to increased capillary permeability, risk for ineffective airway clearance related to laryngeal edema, impaired comfort related to urticaria, and readiness for enhanced health management related to allergy prevention and management.
Now that you have established some nursing diagnoses, it's time to collaborate with Jocelyn and the physician to plan goals for care.
Planning7:50–8:22
By the time Jocelyn is discharged from the ED, she will have adequate cardiac output. Her respiratory edema will resolve, and her respiratory status will continue to improve.
Jocelyn will have less pruritis at the time of discharge, and lastly, Jocelyn will verbalize understanding of strategies to prevent a severe allergic attack, and the importance of keeping her EpiPen with her at all times.
Next, you review the physician's orders and implement your plan of care. You start by administering the ordered IV fluid bolus and the antihistamine diphenhydramine.
Implementation8:22–9:23
Next, you remind her that some symptoms, such as itching, might persist for the next 24 hours, and that the physician recommends that she can continue to take oral diphenhydramine as needed.
You stress the importance of seeking medical attention right away if she experiences worsening of any respiratory symptoms such as shortness of breath or chest tightness, or if there is any continued swelling of her lips or tongue, as these may be signs of a rebound reaction.
Finally, you reinforce the importance of carrying her EpiPen with her at all times. Always wearing her medical alert necklace that notifies first responders about her allergy.
And you review strategies to avoid peanuts hidden in foods, including always carefully reading food labels and avoiding foods that state that they are made on machines where other foods containing peanuts are also made.
Evaluation9:23–10:04
Now, let's check back and evaluate how Jocelyn is doing. Her capillary refill is now less than 2 seconds.
Her heart rate is 85 BPM, and her BP is 118/72 millimeters of mercury. Her respiratory rate is 14 breaths per minute, and she is breathing comfortably with clear lung sounds on auscultation.
Her oxygen has been discontinued, and her SPO2 is 96% on room air. The swelling of her lips and tongue is improving, and she's no longer scratching at her neck and chest.
Jocelyn states that she plans to keep her EpiPen in her purse, and that she will be more careful to avoid exposure to peanuts.
All right. It's a quick recap.
Summary10:04–10:53
Your assigned client, Jocelyn Williams, presented to the ED via EMS with signs and symptoms of anaphylaxis, a severe allergic reaction that affects multiple organ systems.
Your assessment revealed delayed capillary refill, tachycardia, hypotension, swelling of the oral mucosa, wheezing, and pruritis.
Your nursing diagnoses were risk for decreased cardiac output, risk for ineffective airway clearance, impaired comfort, and readiness for enhanced health management.
The goals you identified when planning care included normalizing cardiac output and respiratory status, resolving edema and urticaria, and educating Jocelyn about managing her allergy.
You then implemented your plan and evaluated the effectiveness of her plan of care.
| ANAPHYLAXIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Epinephrine Auto-Injectors for Anaphylaxis Treatment in the School Setting: A Discussion Paper" SAGE Open Nurs (2019)
- "A Clinical Practice Guideline for the Emergency Management of Anaphylaxis (2020)" Front Pharmacol (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Davis Advantage for Townsend’s Essentials of Psychiatric Mental-Health Nursing Concepts of Care in Evidence-Based Practice, Ninth edition" F.A. Davis Company (2022)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)
No notes for this video yet
Try adding a note below